
Saturday, October 2, 2010 - 8:00 AM
17442
Evaluation of Maxillary Alveolar Reconstruction Using a Resorbable Collagen Sponge with rhBMP-2 in Cleft Lip and Palate Patients
Introduction: A resorbable collagen matrix with recombinant human bone morphogenetic protein (rhBMP-2) was compared with traditional iliac crest bone graft for the closure of alveolar defects during secondary dental eruption.
Methods: Sixteen patients with unilateral cleft lip and palate, aged 8 to 12 years, were selected and randomly assigned to group 1 (rhBMP-2) or group 2 (iliac crest bone graft). Computed tomography was performed to assess both groups preoperatively and at months 6 and 12 postoperatively. Bone height and defect volume were calculated through Osirix Dicom Viewer (Apple Inc. Website). Overall morbidity was recorded.
Results: Preoperative and follow-up examinations revealed progressive alveolar bone union in all patients. For group 1, final completion of the defect with a 65.0%-mean bone height was detected 12 months postoperatively. For group 2, final completion of the defect with an 83.8%-mean bone height was detected 6 months postoperatively. Dental eruption routinely occurred in both groups. Clinical complications included significant swelling in three group 1 patients (37.5%) and significant donor-site pain in seven group 2 patients (87.5%).
Conclusions: For this select group of patients with immature skeleton, rhBMP-2 therapy resulted in satisfactory bone healing and reduced morbidity compared with traditional iliac crest bone grafting.
Key words: rhBMP-2, tissue engineering, alveolar bone graft, craniofacial surgery, computed tomography
REFERENCES
1. Bergland O, Semb G, Abyholm F. Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate J 23, 175, 1986.
2. Boyne PJ. Use of marrow-cancellous bone grafts in maxillary alveolar and palatal clefts. J Dent Res 53, 821, 1974.
3. Carstens MH, Chin M, Ng T, et al. Reconstruction of #7 facial cleft with distraction-assisted in situ osteogenesis (DISO): role of recombinant human bone morphogenetic protein-2 with Helistat-activated collagen implant. J Craniofac Surg 16, 1023, 2005.
4. Dickinson BP, Ashley RK, Wasson KL, et al. Reduced morbidity and improved healing with bone morphogenetic protein-2 in older patients with alveolar cleft defects. Plast Reconstr Surg 121, 209, 2008.
FIGURES
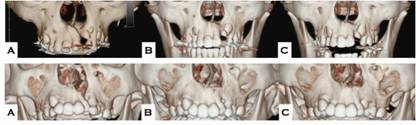
Figure 1 – rhBMP-2 group: A- preoperative, B- 6 months postoperative, C- 12 months postoperative

Figure 2 – Dental eruption
See more of Cranio/Maxillofacial/Head and Neck Paper (5 mins)
Back to 2010am Complete Scientific Program