
Sunday, November 3, 2002 - 8:36 AM
598
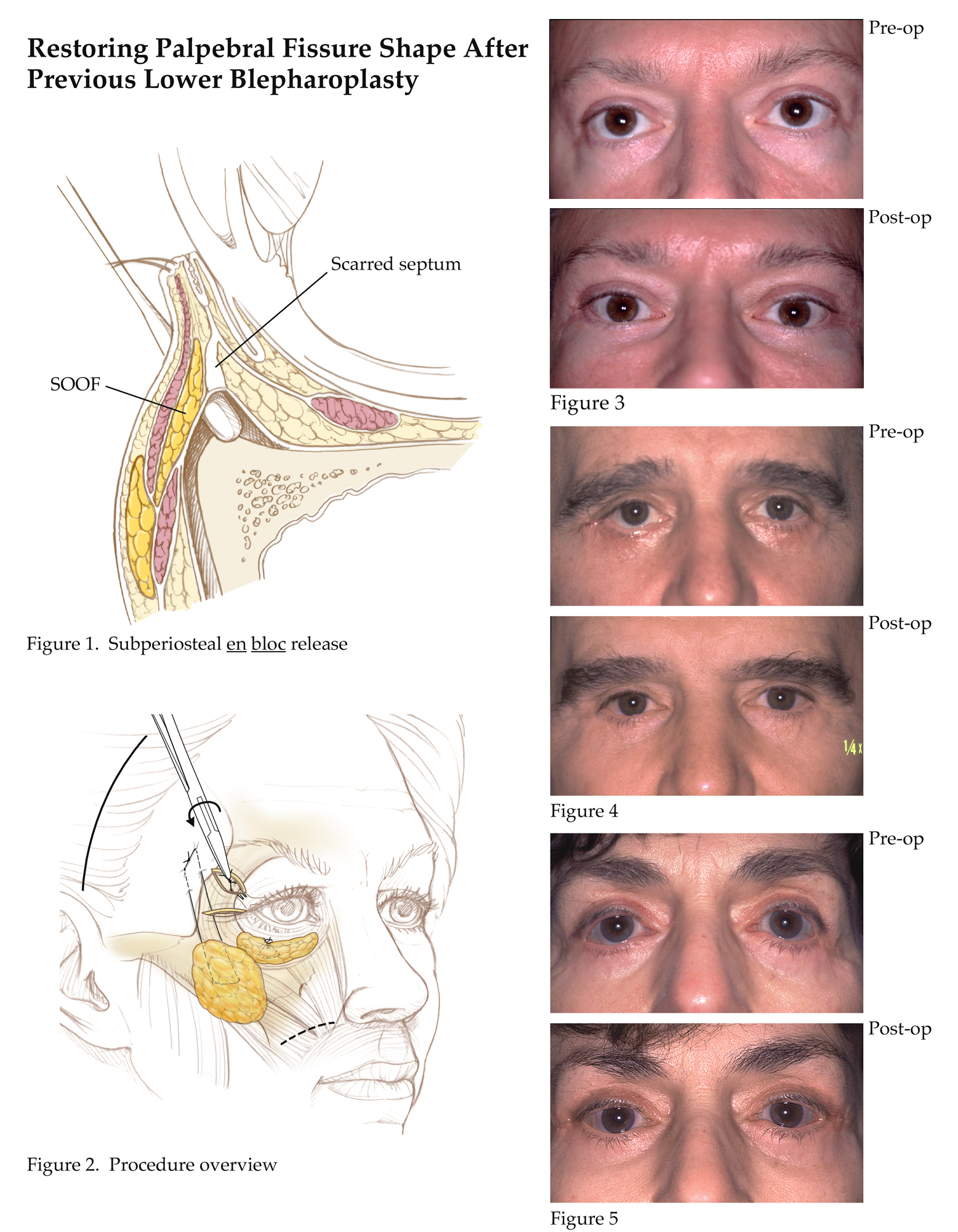
Restoring Palpebral Fissure Shape After Previous Lower Blepharoplasty
Goals/Purpose: Distortion of the palpebral fissure is a frequent sequela after transcutaneous blepharoplasty. A vertical deficiency of the outer lamellae due to over resection and a shortening of the middle lamella from scarring causes the lower lid margin to descend and the lateral canthus to migrate medially, thereby resulting in a “round eye.” Methods: This procedure repositions the lower lid margin and the lateral canthus by separating scarred periorbital, malar midface, and temporal soft tissues from the underlying skeleton by subperiosteal dissection. In effect, a continuous full thickness facial soft tissue flap is created. Vertical elevation and stable fixation of these tissues allows: lid margin to be elevated; recruiting cheek skin to replace deficient outer lamellae; suborbicularis oculi fat to be interposed between the orbital rim and scarred periorbital soft tissues (as a spacer); lateral canthus to be repositioned; and a poor transition between the cheek and temporal area avoided. It avoids the use of interlamellar dissection as well as the use of grafts(Figs. 1,2). Results and Complications: Lower lid position and palpebral fissure shape have been restored in a series of 15 patients operated on over a six year period. Three of the patients required revision of their canthopexy. In eight patients who had complaints of “dry eye,” four had significant improvement, and four had resolution of their symptoms(Figs. 3,4,5). Conclusion: Subperiosteal en bloc release and elevation of the midface, lid lamellae, and lateral canthus with secure fixation to the bony orbit can effectively restore palpebral fissue shape after previous lower lid blepharoplasty. It has the advantages of:1)avoiding skin or posterior lamellar grafts; 2)avoiding interlamellar dissection; 3)avoiding canthoplasty and its concomitant reduction in the width of the palpebral fissure and distortion of the lateral commissure; 4)avoiding soft tissue redundancy in the temporal area; 5)restoring the cheek/lid interface.
View Synopsis (.doc format, 239.0 kb)
See more of Cosmetic
Back to 2002 Complete Scientific Program
Back to 2002 Meeting home