
Monday, November 4, 2002
1038
Biplanar Concepts in Endoscopic Internal Augmentation Mammaplasty
Introduction: The author describes a new technique which allows application of transaxillary endoscopic methods to correct advanced breast ptosis using biplanar concepts. Breast tissue dynamics can now be modified internally without skin excision techniques.
Materials and Methods: The author details a 6-year experience in 32 patients using endoscopic techniques for augmentation in patients with breast ptosis, as a subset of an overall 10-year experience in over 400 patients who underwent endoscopic augmentation mammoplasty. Patient selection criteria included mild to severe second-degree ptosis (nipple being below the inframammary fold but not at the apex of the breast n=26 or tubular type breast deformity n=6)).
Technique: Four different endoscopic methods are described: 1) Endoscopic Partial Biplanar (EPB), 2) Endoscopic Full Biplanar (EFB), 3) Endoscopic Trans-Muscular (ETM) and 4) Endoscopic Transmuscular with intra-parenchymal Mammoplasty (ETM-M). Techniques 1, 2 and 3 are for increasing levels of ptosis and 4 is for ptosis with tubular type deformity. Appropriate candidates for each technique will be described and endoscopic methods demonstrated in both the submammary (Fig. 1) and the sub-muscular (Fig. 2) planes (Fig. 3). These applications will be outlined and postoperative results will be shown (Example 1-3).
Results/Complications: Patient satisfaction was 100% due to the lack of external scars on the breast. Four patients sustained a segmental loss of sensation in the lower, outer breast. These patients required intra-parenchymal dissection. Sensation returned in three patients and one was lost to follow-up.
Conclusion: Endoscopic internal augmentation mammoplasty using biplanar concepts may help avoid skin excision techniques in certain patients with breast ptosis and tubular type deformity.
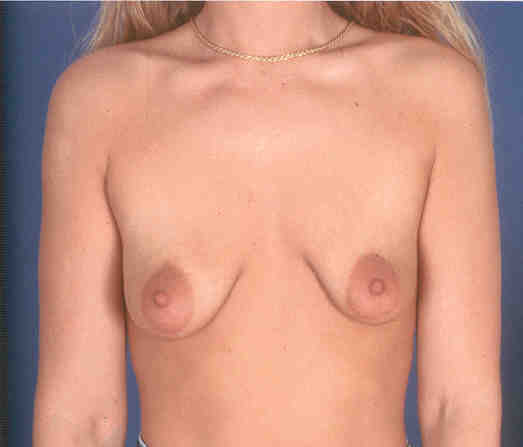
Example 1
Preop


Postop



Example 2
Preop



Postop



Example 3
Preop



Postop
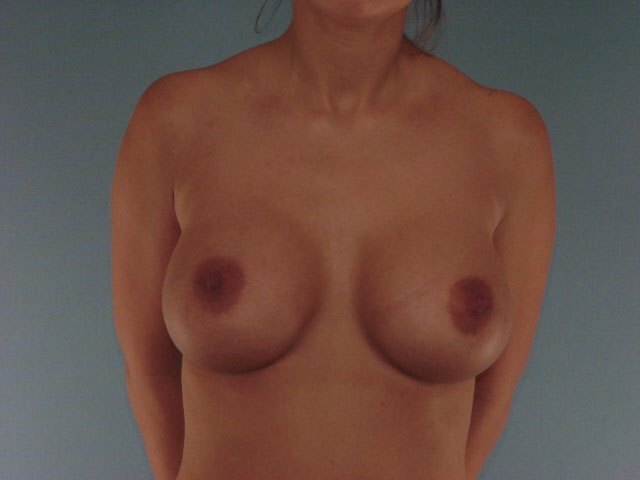

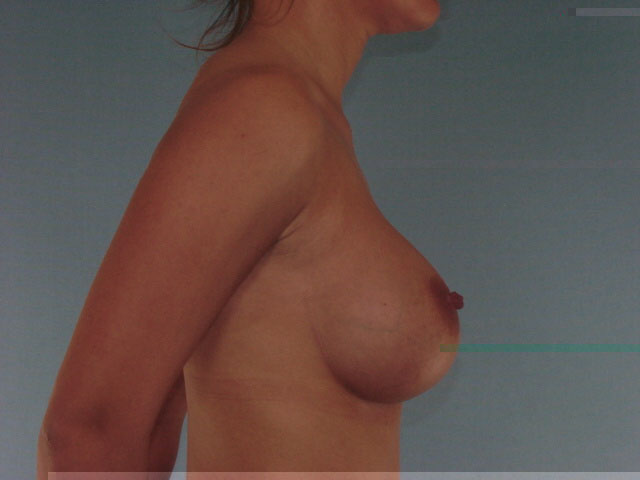
Fig 1 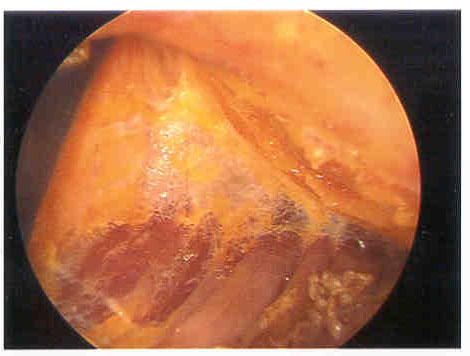
Fig 2 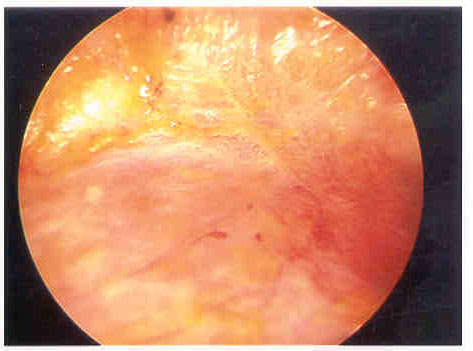
Fig 3 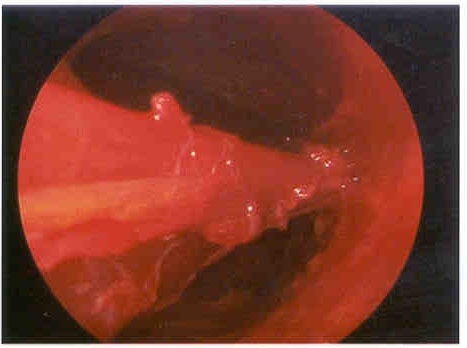
See more of Breast (Cosmetic and Reconstructive)
Back to 2002 Complete Scientific Program
Back to 2002 Meeting home