
Sunday, November 3, 2002
1048
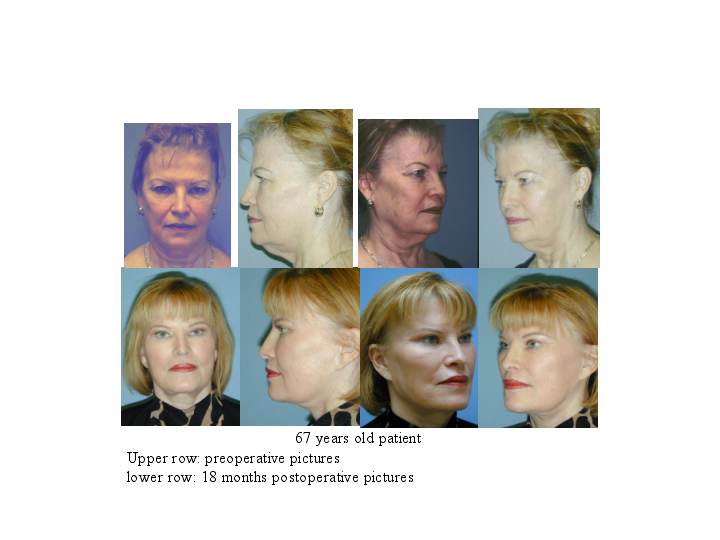
A Differential Approach to the Midface Lift: An Anatomic and Clinical Study
The midface lift has been employed as an additional tool in facial rejuvenation. The procedure is predicated on the concept that gravitational effects in older patients result in descent of the mid-face soft tissues. This leads to a gradual thinning of the tissue over the inferior orbital rim and an associated “ tear trough” deformity, deeping of the nasolabial folds, and jowling deformity. These are partially improved with classical approaches (fat conserving blepharoplasty, the muti-layered rhytidectomy, and augmentation. The midface lift addressed these problems directly but is employed with reluctance because of an associated increase in morbidity) and the potential for complications involving the lower eyelid. We have modified this technique utilizing either a curved lateral temporal incision within the hairline, an extended blepharoplasty incision, or a combination of both. In the temporal approach, a subperiosteal dissection is performed over the superior, lateral and inferior orbital rims with the dissection completed via an intra-oral incision- fully mobilizing the midface subperiosteally. Two 2-0 Nylon sutures are placed in the deep cheek mass, passed under the elevated malar and temporal soft tissues and out through the lateral temporal incision. Both sutures are placed under appropriate tension to secure the cheek, corner of the mouth and fixed to a 6mm titanium screw placed over temporal line. After securing a symmetrical cheek elevation the temporal incision is closed without excising skin by rotating the inferior hair-bearing skin flap anteriorly to secure a lateral brow lift. If a blepharoplasty approach is employed, the subperiosteal dissection is over the entire zygomatico-maxillary complex, without a buccal incision. Suture stabilization is to a 6mm titanium screw inserted into the lateral orbital rim. Occasionally, both the temporal and blepharoplasty exposures are appropriate. The indications for each of these 3 modifications will be discussed. The presentation will include a series of 17 patients, 44 to 69 years old who were followed from 2 to 26 months, (mean follow-up 9 months) included in this group are three patients with facial nerve paresis in whom lateral oral commissure drooping and cheek sagging were problems. Additionally, results from fresh cadaver specimen dissections are included to demonstrate the differential effects of variations in suture placement and suspension. Through this approach to the midface lift, the morbidity frequently associated with this procedure has been reduced and the complications described above have been avoided.
See more of Cosmetic
Back to 2002 Complete Scientific Program
Back to 2002 Meeting home