
Tuesday, October 28, 2003
3604
The "Pinch" Lower Blepharoplasty:Revisited
Purpose:
The goal of this clinical study was to evaluate the efficacy of a combined transconjunctival and transcutaneous lower blepharoplasty approach to more effectively preventing postoperative scleral show or ectropion while still delivering an equally satisfactory or even superior aesthetic improvement, as compared to the traditional skin-muscle flap technique.
Methods/Techniques:
This combined approach blepharoplasty was performed on all patients who were candidates for eyelid rejuvenation, from July 1, 2001 until March 1, 2003. At least 6 months follow up was required for all patients. There were a total of 53 patients.
The surgical technique initially includes the delivery of conscious sedation anesthesia using Versed and Fentanyl. This step is critical because the sedation allows the surgeon to judge and pre-mark not only the upper but also the lower eyelid skin excess, just before the local anesthesia must be placed.
The excision of excess skin is conducted after the transconjunctival removal of excess fat since the amount of redundant skin can potentially be less, particularly in cases where significant redundant fat is extracted.
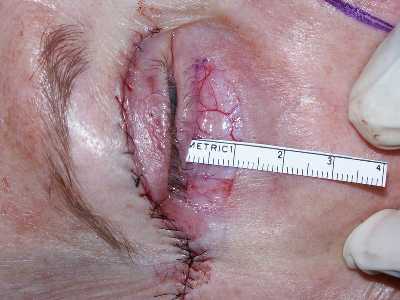
Using two fine brown adson forceps, the excess skin is firmly pinched, guided by the pre-markings, creating a "wall" of skin. The posture of the lower eyelid is observed to insure that there is no downward drawing of the lid margin. Should this happen, then the amount of excess skin pinched can be reduced. This critical pinch simulates the tension eventually produced by the suture closure of the lower eyelid wound. A straight scissors is then used to excise the "wall" of skin.
Closure of the lower eyelid wound is performed with a 7-0 nylon suture. Steri-strip taping is usually unnecessary. Sutures are removed within 4 to 5 days. Routine eye drops and ointment is ordered and again, no taping is usually necessary post-operatively.
It should be noted that the same surgeon (the author) performed all surgeries. The cases were then reviewed, at least 6 months and as much as 18 months post operatively.
Results/Complications:
Of the 40 blepharoplasties performed, there were no significant postoperative cases of scleral show and no cases of frank ectropion. This encouraging finding was paired with the fact that more redundant skin could be removed safely by the pinch technique and the results were often commensurately better than the traditional skin-muscle approach.
It should also be noted that by avoiding elevation of a skin-muscle flap, there was noticeably less bruising and swelling post-operatively with this technique. None of the patients required postoperative taping or prolonged use of eye drops or ointment.
This approach was applicable to all blepharoplasty patients, whether primary or secondary.
Conclusions:
The "pinch" blepharoplasty has proved to perhaps be a superior approach for the removal of excess lower eyelid skin and fat. This advantage is probably secondary to the fact that the orbicularis muscle and orbital septum are not violated and a heavy skin muscle flap is not created. This approach allows for efficient and consistent removal of both the excess fat and skin without the attendant and almost expected incidence of some postoperative scleral show or even short-term ectropion, with the traditional skin-muscle technique.
|
Preoperative |
Postperative |
|
Preoperative |
Postperative |
|
Preoperative |
Postperative |
|
Preoperative markings |
Pinch technique |
|
Excision technique |
Excision |









View Synopsis (.doc format, 9133.0 kb)
See more of Cosmetic
Back to Plastic Surgery 2003 Complete Scientific Program
Back to Plastic Surgery 2003 Meeting home