
Wednesday, October 29, 2003
3953
P54: Low Height Tissue Expanders Produce a more Aesthetic Breast Shape in Post-Mastectomy Implant Reconstruction
Staged post-mastectomy breast reconstruction with conventional (full height) tissue expanders and subsequent implant placement often produces shortcomings related to breast shape due to excessive upper pole fullness. To address this we have used a short height (McGhan 133 LV) tissue expander for most of our breast reconstructions over the past 24 months. We sought to analyze and compare the breast shape produced by this tissue expander with that resulting from the use of the full height device.
Using a computer assisted digital photographic analysis we compared the upper pole breast shape in 14 consecutive patients who underwent implant breast reconstruction following tissue expansion. Seven patients underwent expansion with conventional, full height expanders (Group 1) and in 7 patients we used a short height expander (Group 2). All patients had subsequent reconstruction with a textured shaped silicone gel implant. Each breast was photographed in the 90 degree lateral position (reconstructed breast facing the camera) at 3 feet with a 2.5 megapixel digital camera (Olympus, Camedia) and the lens focal length set to 28mm. The image width was standardized to 4cm and the height to 11.4-11.6cm using Adobe PhotoShop 7. The mean follow-up was 10 months with a range of 6-22 months.
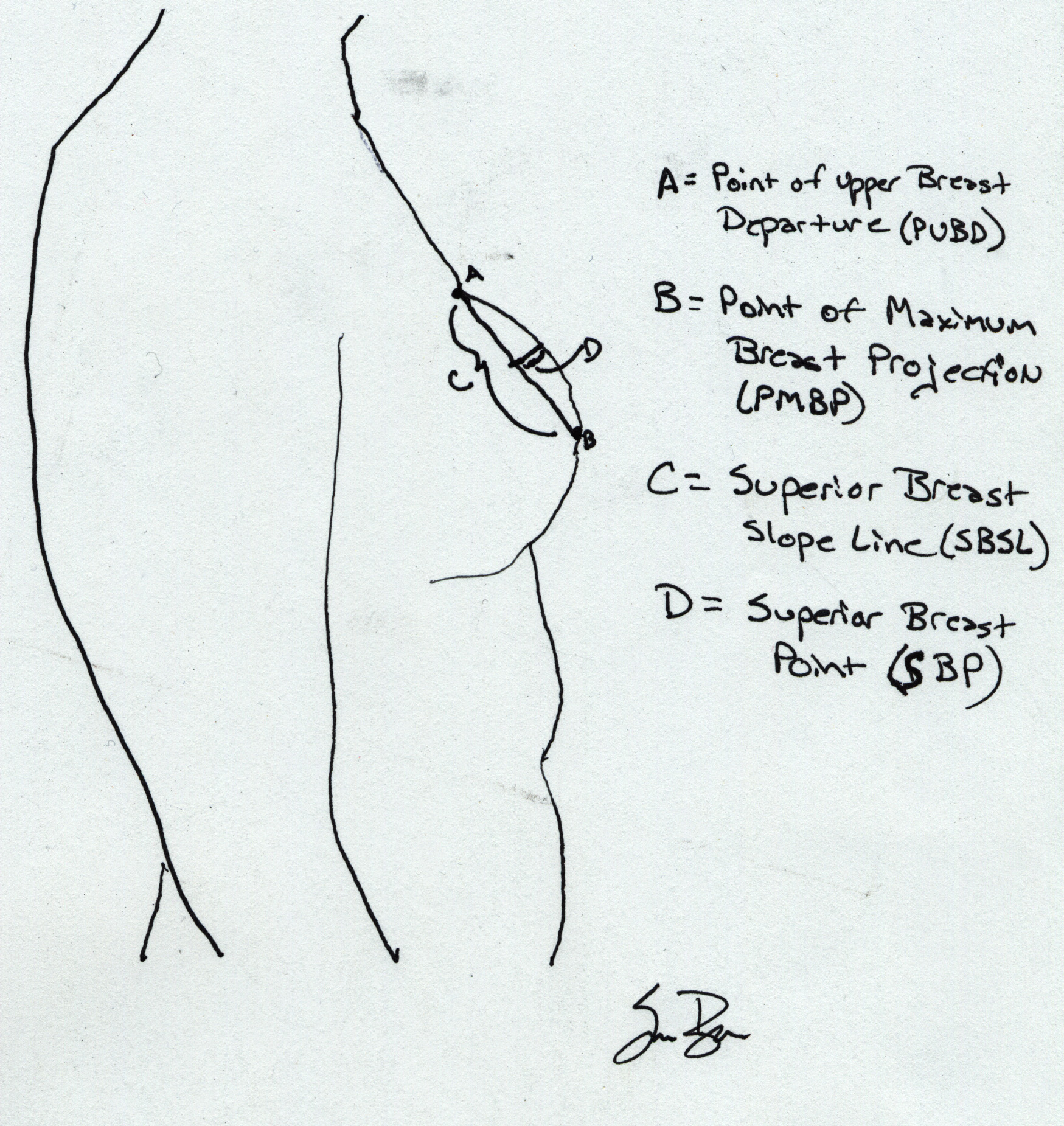
The superior breast slope line (SBSL) was created by joining the point of upper breast departure from the chest wall (PUBD) with the point of maximum breast projection (PMBP) as in Figure 1. The distance of a perpendicular line drawn from the mid-point of SBSL to the actual breast skin edge defined the superior breast point (SBP). The SBP values in Group 1 were compared to those in Group 2 using the paired Studentĺs t-test.
The mean SBP in the breasts reconstructed using preliminary low height expansion devices was 1.92mm (SD=.416mm) while the mean SBP produced by previous expansion with full height expanders was 3.86mm (SD=.789mm). The mean SBP in the low height expanded breasts was significantly lower than that of the full height expanded breasts ( p< .0001).
Our study confirms the fact that low height tissue expanders produce a better upper pole breast shape. We believe that this is because expansion occurs in the lower pole tissues only. Upper pole tissues are not appreciably expanded or stretched. Using a simple superior capsulotomy and limited sub-muscular dissection at the second stage (expander removal and implant placement) the surgeon can predictably produce an aesthetically pleasing, tapered fullness of the upper pole without excessive fullness which is more often seen when conventional full height breast tissue expanders are used.
See more of Posters
Back to Plastic Surgery 2003 Complete Scientific Program
Back to Plastic Surgery 2003 Meeting home