
Sunday, October 10, 2004 - 7:30 AM
6009
An Anatomic Evaluation and Surgical Approach to the Perioral Mound in Facial Rejuvenation
An Anatomic Evaluation and Surgical Approach to the Perioral Mound in Facial Rejuvenation
Objective:Ā The anatomic stigmata of aging in the perioral area is a complex expression of soft tissue changes, particularly adjacent to the nasolabial folds. Patients are critical in identifying this perioral fullness as a dissatisfying product of aging. At the same time,Ā rejuvenation of this area can be challenging to achieve ideal results with longevity, often vulnerable to early relapse after facial rejuvenation procedures.Ā To better understand the elements impacting on this vital structural framework, we undertook an investigation of the perioral region.Ā A surgical approach is justified through this anatomic appreciation.
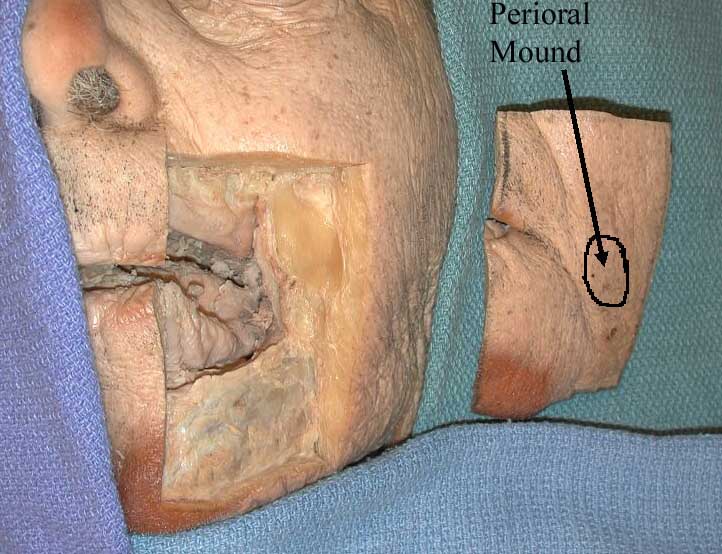
Methods: ĀEight fresh and fixed cadavers with obvious perioral fullness were identified with subsequent harvesting ofĀ 6x6 cm composite block specimens encompassing the nasolabial fold, oral commissure and identified perioral fullness (Figure 1). Histologic sectioning was performed in two planes (vertical and horizontal) at multiple levels and subsequently stained with Hematoxylin-Eosin as well as Elastin-Trichrome.
Surgically the perioral mound is marked preoperatively (Figure 2a,b,c). The perioral mound is approached from two directions with a 1.5mm liposuction canula during facial rejuvenation.Ā
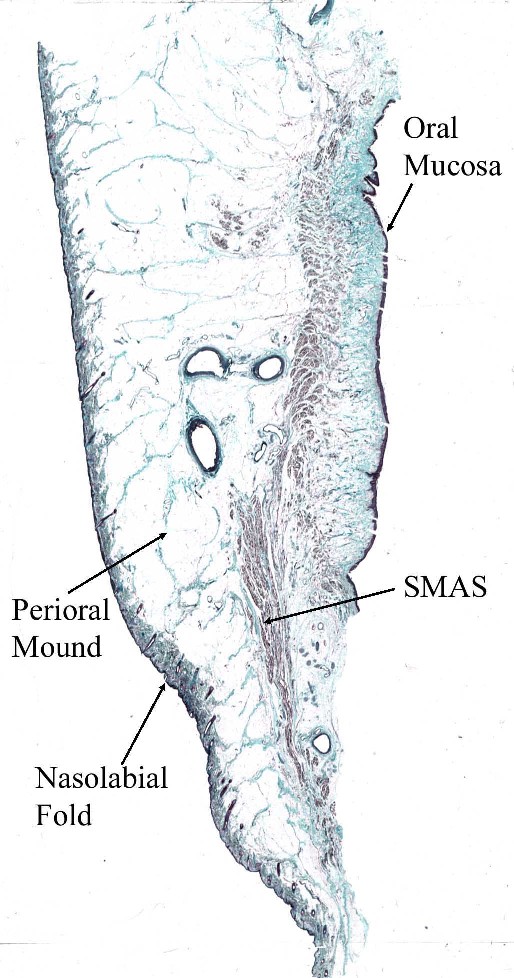
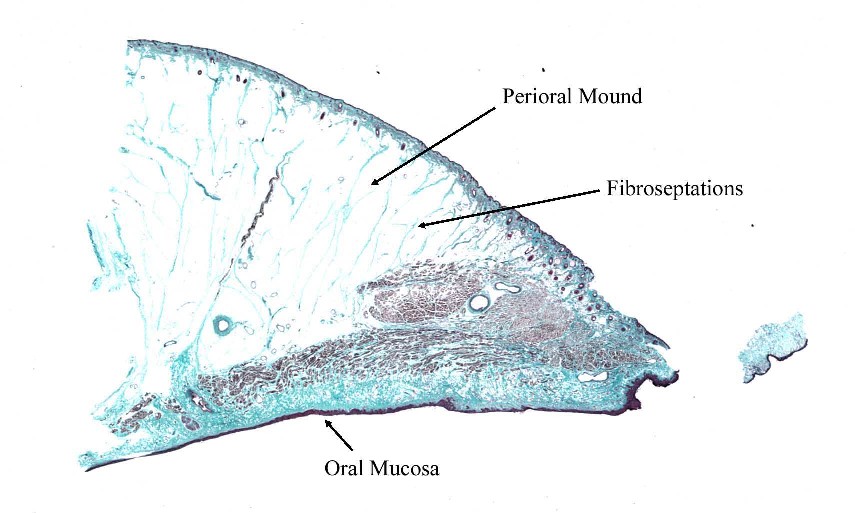
Results:Ā Histologic sections of the perioral region were remarkable for a lipomatous area without defined ligamentous attachments or encapsulations. There were chambers of adipocytes separated by thin fibroseptations in the hypodermis. The connective tissue septa, or retinacula,Ā serves as a scaffold of structural support in this region (Figure 3 & 4).Ā A musculoaponeurotic layer is deep to this area, and becomes more organized caudally and medially within the specimens.Ā This SMAS layer may buttress the superficial lipomatous tissue as it descends inferiorly, such that the volume is displaced anteriorly producing projection and elevation in the respective perioral area. Nonetheless, there is a clear superficial lipodystrophy which defines the clinical findings in the cadaver specimens.
Conclusions: The characterization of the histologic components of the perioral region will enable the plastic surgeon to more thoroughly understand this area during facial rejuvenation.Ā The perioral mound demonstrated in this area is amenable to conservative contouring with liposculpturing during rhytidectomy procedures to optimize perioral rejuvenation.Ā (Figure 2d, e)
|
|
|
| Fig 1 | Fig 2a |
|
|
|
| Fig 2b | Fig 2c |
|
|
|
| Fig 3 | Fig 4 |
|
|
|
| Fig 2d | Fig 2e |





| |||||||
| |||||||
| |||||||
| |||||||