
Wednesday, September 28, 2005 - 7:45 AM
8086
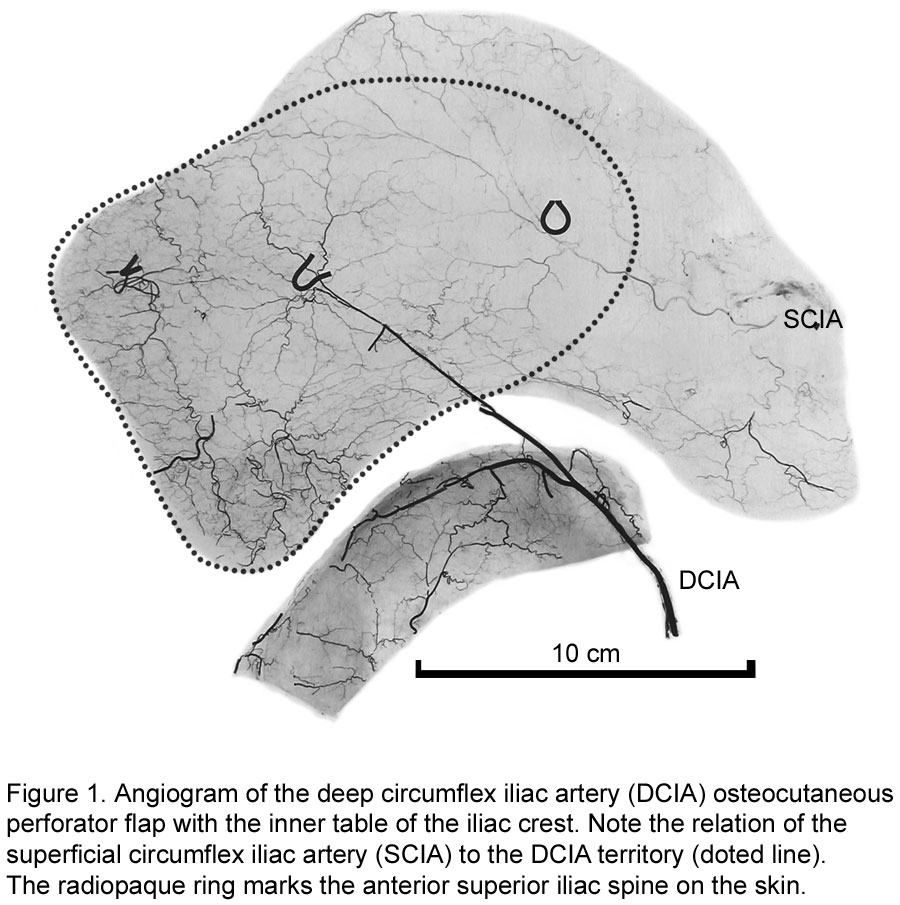
The Anatomical Basis of the Deep Circumflex Iliac Artery Perforator Flap
Introduction: Flaps containing a large segment of bone along with a cutaneous paddle on a single vascular pedicle are few. The deep circumflex iliac artery (DCIA) iliac crest osteocutaneous flap is a well known flap for mandibular reconstruction because of its long pedicle, large diameter and reliable vascularity. The traditional design of the flap included an obligatory abdominal muscle cuff to include perforators to the overlying skin, which resulted in undesirable bulk. Published accounts of the location, size and number of DCIA perforators are contradictory. Limited clinical success has been achieved with the DCIA perforator flap with iliac crest. The purpose of the current study is to comprehensively document the anatomical basis of the DCIA osteocutaneous perforator flap. Methods: Six fresh cadavers underwent whole body injection with a mixture of lead oxide and gelatine. All skin perforators in the lateral trunk and upper thigh region were dissected by layer, documenting their course to their respective source arteries using angiography and photography. The contribution of the DCIA to the iliac bone, the location of the cutaneous perforators with respect to the iliac crest and the skin territory supplied by each perforator was measured with Scion Image beta 4.02 for Windows. Results: An average of 1.6 DCIA cutaneous perforators were present in 92% of dissections. They were found in a 3.5 by 5cm region, located on the superior aspect of the iliac crest, 5 cm posterior to the anterior superior iliac spine. The average internal diameter was 0.7mm and the pedicle length to the deep fascia was 1.3cm. The average cutaneous perforator zone was 31cm2 and the angiosome surface was 54cm2. The average length of the pedicle for the DCIA perforator flap alone was 11.4 cm. The average DCIA arterial pedicle length for the osteocutaneous perforator flap was 4.6 cm long and 2 mm in diameter. DCIA perforators can be differentiated from intercostals and lumbar perforators during a superior to inferior dissection as they do not travel with a cutaneous nerve. The DCIA provides vascular supply to the segment of iliac crest used in mandibular reconstruction for its entire length directly and via a rich anastomotic network with the iliolumbar or lumbar artery. A flap design including only the inner table of the iliac crest preserves this vascular network, and would potentially decrease donor site contour deformity associated with bilaminar iliac crest resection. Conclusion: The DCIA perforator osteocutaneous flap provides a significant improvement over the previous iliac crest flap since it is less bulky, provides improved versatility and has reliable vascularity.
View Synopsis (.doc format, 127.0 kb)
See more of Hand, Upper Extremity/Microsurgery
Back to 2005am Complete Scientific Program