McCormick Place, Lakeside Center
Sunday, September 25, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Monday, September 26, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Tuesday, September 27, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Wednesday, September 28, 2005
9:00 AM - 5:00 PM
8140
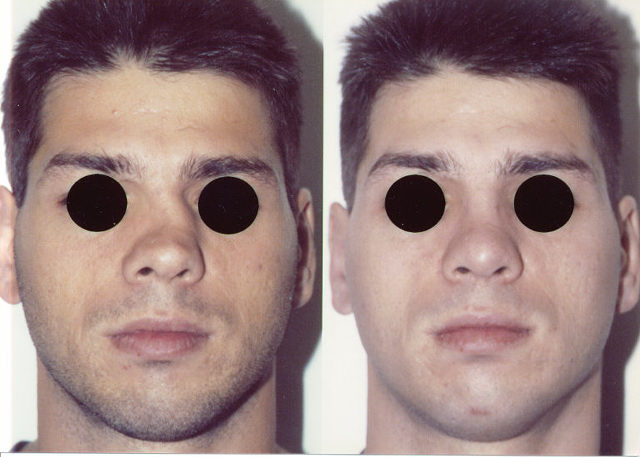
The Role of High Septal Osteotomy in the Management of the Deviated Nose
The deviated nose represents a complex functional and cosmetic problem. For reliable correction all components contributing to the deformity must be addressed. Because of the septum's intimate relationship to the soft tissues, upper and lower lateral cartilages and nasal bones, septoplasty plays a crucial role in nasal straightening. When attempting to correct a patient's crooked nose that does not require dorsal hump resection, medial and lateral osteotomies with infracture are routinely performed. Such osteotomies succeed in mobilizing the nasal sidewalls but neglect the central septal structure of the upper nose. This structure (which is flexible) may hinder the stable midline reduction of the bony nasal pyramid and lead to post operative nasal drift. We describe High Septal Osteotomy to provide a controlled septal cut which mobilizes the central structure. After performing a submucous resection, the cartilaginous septum is separated from the ethmoid plate posteriorly and from the vomer inferiorly. Release of posterior and inferior septal attachments allows the cartilaginous dorsal septum to rotate towards the midline when the bony septum and nasal bones are reduced It is important to preserve the attachment of the cartilaginous septum to the bony septum at the keystone area to avoid loss of septal support. After dorsal nasal the upper lateral cartilages are sharply detached from the cartilaginous septum. Osteotomies are performed beginning with intermediate osteotomies when required. Bilateral medial osteotomies are performed by advancing the osteotome parallel to the septum on each side until the old fracture line is reached, and then curving laterally on each side. The lateral osteotomy must connect with the medial osteotomy to fully mobilize the nasal sidewall. Once the nasal side walls have been mobilized, the high septal osteotomy is performed to permit midline reduction of the nasal dorsum. A single-guarded curved osteotome is introduced into the window provided by the septal resection, engaging the posterior septum at the level of the dorsal strut (usually 1 to 2 cm below the dorsum). The guard is placed on the side of mucosal elevation with the curve oriented upward (the left-guarded osteotome is chosen if the left mucosa has been elevated). With the skin protected, the osteotome is advanced until it emerges entirely through the bony dorsum just below the nasion
This technique was utilized for twenty-six patients; twenty-five of whom had excellent results. This maneuver permitted stable midline reduction of the nasal pyramid without dorsal collapse.