
Sunday, September 25, 2005 - 1:25 PM
8154
Disarticulated Fascial-Fat Grafts Offer Superior Viability and Constancy Compared to Fat Injection for Facial Filling: Clinical, Histologic and 3-D CT Correlation
Goals: ĀĀCompare viability of fat injection specimens with disarticulated fascial-fat grafts using histology, trypan blue tests, and 3-D CT scans.Ā Demonstrate clinical examples of disarticulated fascial-fat grafting.
Clinical Technique:Ā ĀĀDisarticulated fascial-fat grafts were harvested from the suprapubic region in 120 patients.Ā Grafts are cut into 1-2 mm strips, and structural connections (Scarpa's fascia, fatty septae) are cut (disarticulated) and retained on cool moist Telfa gauze until the time of transplantation.Ā Subcutaneous pockets are created in the nasolabial complex, Marionette complex, upper and lower lips, lateral perioral commissures, cheeks, malar eminences, submalar region, temporal hollowing, glabella, and eyebrow.Ā Grafts are inserted through adjacent stab incisions.Ā
Histology:Ā Fat injection specimens were obtained using the Coleman fat aspiration canula and centrifuged.Ā Disarticulated fascial-fat grafts and fat injection specimens were Āharvested and subjected to trypan blue exclusion studies,Ā stained (H & E) staining and analyzed at 40X, 100X, and 430X magnification for cellular wall integrity, nuclear exclusion of trypan blue, nuclear shape.Ā Viability in both groups are quantified.
3-D CT scans:Ā Three dimensional CT scans performed on a Siemens CTI Reveal XVI CT Scanner.Ā Computer-generated 3-D reconstructed images were obtained on select patients.Ā Before-after patient photographs and 3-D CT scans are compared with respect to soft tissue measurements, a measure of graft take.
Clinical Results: 119 consecutive patients underwent disarticulated fascial-fat grafts to the face.Ā One to eight areas were transplanted.Ā Grafts are inserted readily and immediate postoperative swelling is less than that with fat injection.Ā Follow-up is 6-48 months. Minor complications included two wound infections (treated with cephalosporin antibiotics and local wound care (all grafted material survived), visibility of infraorbital grafts (6 patients overall with larger fill volumes) and a 6% revision rate (4 in the infraorbital region for slight visibility of grafts), 2 for minor asymmetries. 3 patients required minor revisions of the recipient stab incision.Ā
3D CT Scan Results:Ā Disarticulated fat-fascial grafts) provide demonstrable, even three dimensional filling of the face.Ā
Histologic results: Viability of fascial-fat grafts is compared with that of fat injection specimens by trypan blue exclusion and H & E staining.Ā Fascial-fat grafts:Ā 78%-100% (mean 88%) by trypan blue vital exclusion dye and histologic studies.Ā Viability of fat injection ranges from 0% to 55%, (mean 25%) as determined by nuclear exclusion of trypan blue and pyknosis of nuclei (indicating cell death).Ā At 430X magnification, cellular wall disruption is routinely seen in fat injection but not in harvested fascial-fat grafts.Ā An abundance of fibrous tissue (30%) is observed in fascial-fat graft specimens.Ā Fat injection viability is highly variable, with pockets of moderate viability interspersed with pockets of low or no viability.
Conclusions:Ā Fat-fascial grafts provide superior viability to fat- injection specimens.Ā
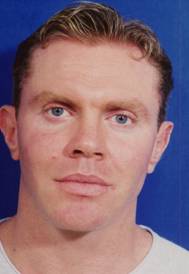
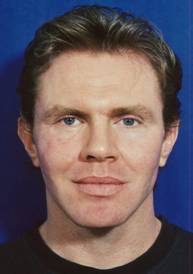
Clinical Examples:Ā All photographs represent a single surgical session with no repeat transplantations.




Fascial-fat grafts to the malar eminences, nasolabial folds, lips, marionette complex, jawline, in combination with a rhytidectomy




Large volume single stage fascial-fat grafts to malar eminence, cheeks, nasolabial fold, lateral perioral commissures, infraorbital region




Fascial-fat grafts to malar eminences, cheeks, lips, lateral perioral commissures in combination with a rhytidectomy


Intraoperative photographs showing immediately prior to and following fascial-fat graft transplantation


Correction of right sided posttraumatic infraorbital enophthalmos with fascial-fat graft




Fascial-fat grafts to under eye area, nasolabial folds, Marionette line in combination with a rhytidectomy






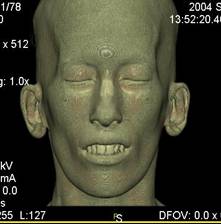
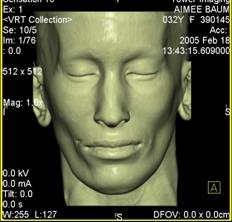
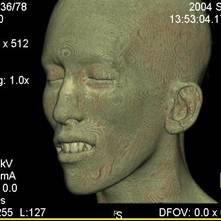
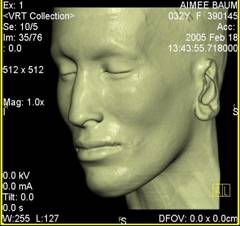
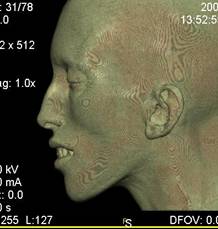
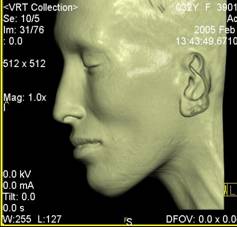
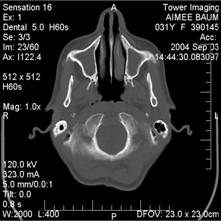
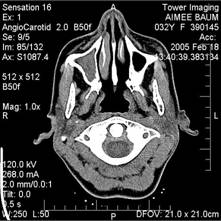
3-Dimensional CT Scans of patient with fascial-fat grafts to malar eminence, submalar region, perioral region, upper and lower lips Increased soft tissue above bony landmarks demonstrates % increase in thickness of soft tissue window at submalar level.
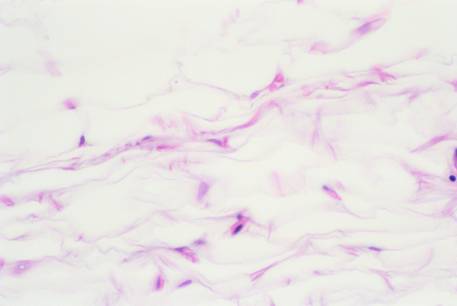
Photomicrograph of harvested fascial-fat tissue at 430X magnification (H and E stain).Ā Note healthy nuclei and intact cellular wall structure.Ā Cell nuclei have excluded trypan blue.
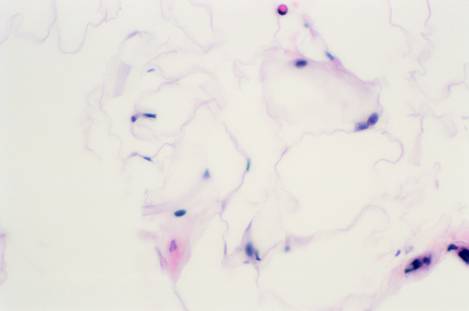
Photomicrograph of fat injection harvest specimen.Ā Note cellular wall disruption and pyknotic nuclei, which have allowed entrance of trypan blue vital dye.Ā
View Synopsis (.doc format, 32.0 kb)