
McCormick Place, Lakeside Center
Sunday, September 25, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Monday, September 26, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Tuesday, September 27, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Wednesday, September 28, 2005
9:00 AM - 5:00 PM
8374
External Cranial Distraction With MCDO System
Inrtroduction: The distraction osteogenesis has been widely accepted to the facial skeletal deformities, however, its application to craniosynostosis is still controversial. Internal cranial distraction procedure has been performed in our unit for the treatment of selected 21 cases of craniosynostosis since 1996. That led us to the conclusion that two disadvantages diminished the benefit of cranial distraction. One is the limitation of deformed skull reshaping with unidirectional distraction device, and the other is the need for a second operative procedure to remove the implanted distraction devices. In order to solve these problems we have designed new distraction system, which is multidirectional cranial distraction osteogenesis (MCDO) system.
Material and methods: Since 2002, we have performed this new method for 11 cases of syndromic and non-syndromic craniosynostosis. Basic maneuver is the same as previously reported distraction procedure, however, calvarium is osteotomised in 9 to 15 small rectangular pieces of bone. The bone flaps are not dissected from the dura, so that vascularity of each bone flap is left intact. The tiny pins are fixed on the temporal bone and the bone flaps. After closing the wound as the pins are penetrating the scalp, the helmet-like flame is then fixed on the pins in temporal bone. The wires tied with each pin on bone flap are passed through halls in the flame as the bone flaps would be pulled in adequate direction. Finally the wires are fixed to the distractors attached on the flame. Distraction is initiated 5 days postoperatively, and continued until the desired skull shape is achieved by controlling the amount of distraction of each bone flaps. The flame and all pins are removed after 3 weeks consolidation period under sedation.
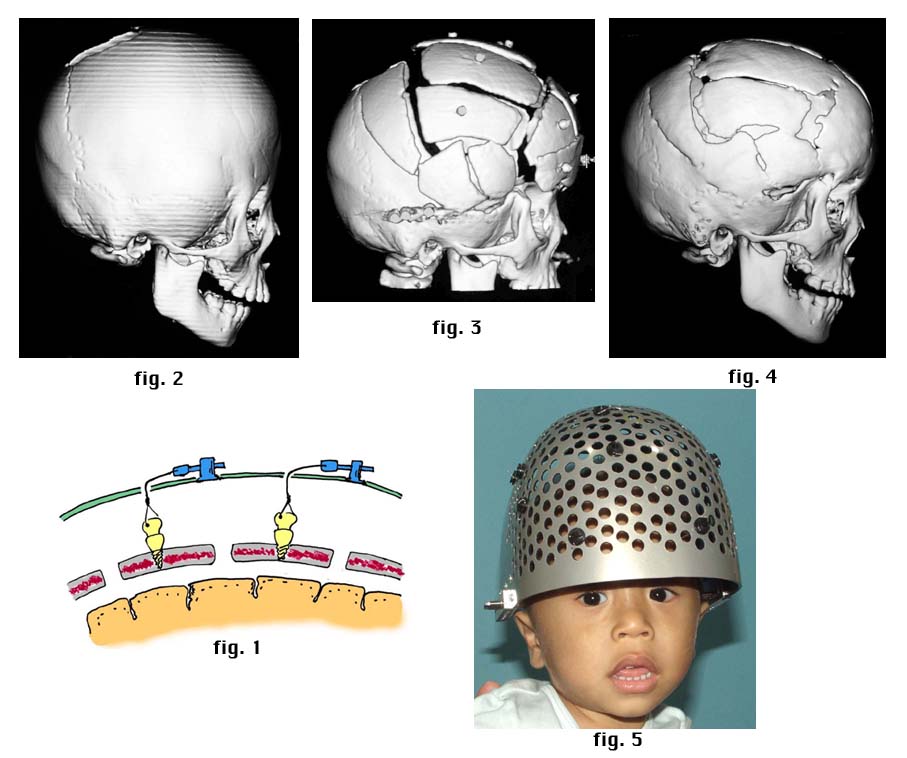
Case Report: A 4-year-old girl with Pfeiffer syndrome underwent cranial distraction with MCDO system. The bone flap was pulled with wire by activating the distractor (fig. 1). Preoperative (fig. 2), before removal of devices (fig. 3), and 20 months postoperative 3DCT (fig. 4). MCDO system is easy to manage at home (fig. 5).
Results: There were no neurologic findings during distraction. No meningitis, liquoric fistula, or extradural hematoma developed. Loosening of pins and pin-track infections occurred in 7 and 6 of 11 cases. The mean total blood transfusion (intra- and postoperative) was 29ml/kg, which is in contrast to the transfusion requirements for the more extensive operations (58.9ml/kg). The longest follow up was 21 months. There was no detectable relapse in any of 11 cases.
Discussion: The advantages of distraction osteogenesis in the field of craniofacial surgery are widely accepted. Refinement of distraction devices is extending its application to various kinds of craniofacial malformations. MCDO system is a type of external distraction device including the following advantages: 1) multidirectional skull contouring is possible with distraction osteogenesis; 2) a second surgery is much less invasive than internal distraction device; 3) leaning curve of surgery is acute; 4) it is applicable to secondary cranial expansion with multiple skull defects. MCDO system allows us to contour various kinds of skull deformities with ease under the concept of cranial distraction.
View Synopsis (.doc format, 17.0 kb)