
McCormick Place, Lakeside Center
Sunday, September 25, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Monday, September 26, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Tuesday, September 27, 2005
9:00 AM - 5:00 PM
McCormick Place, Lakeside Center
Wednesday, September 28, 2005
9:00 AM - 5:00 PM
8488
Thoracodorsal Artery Perforator Flap for the Treatment of the Axillary Hidradenitis Suppurativa
|
| ||
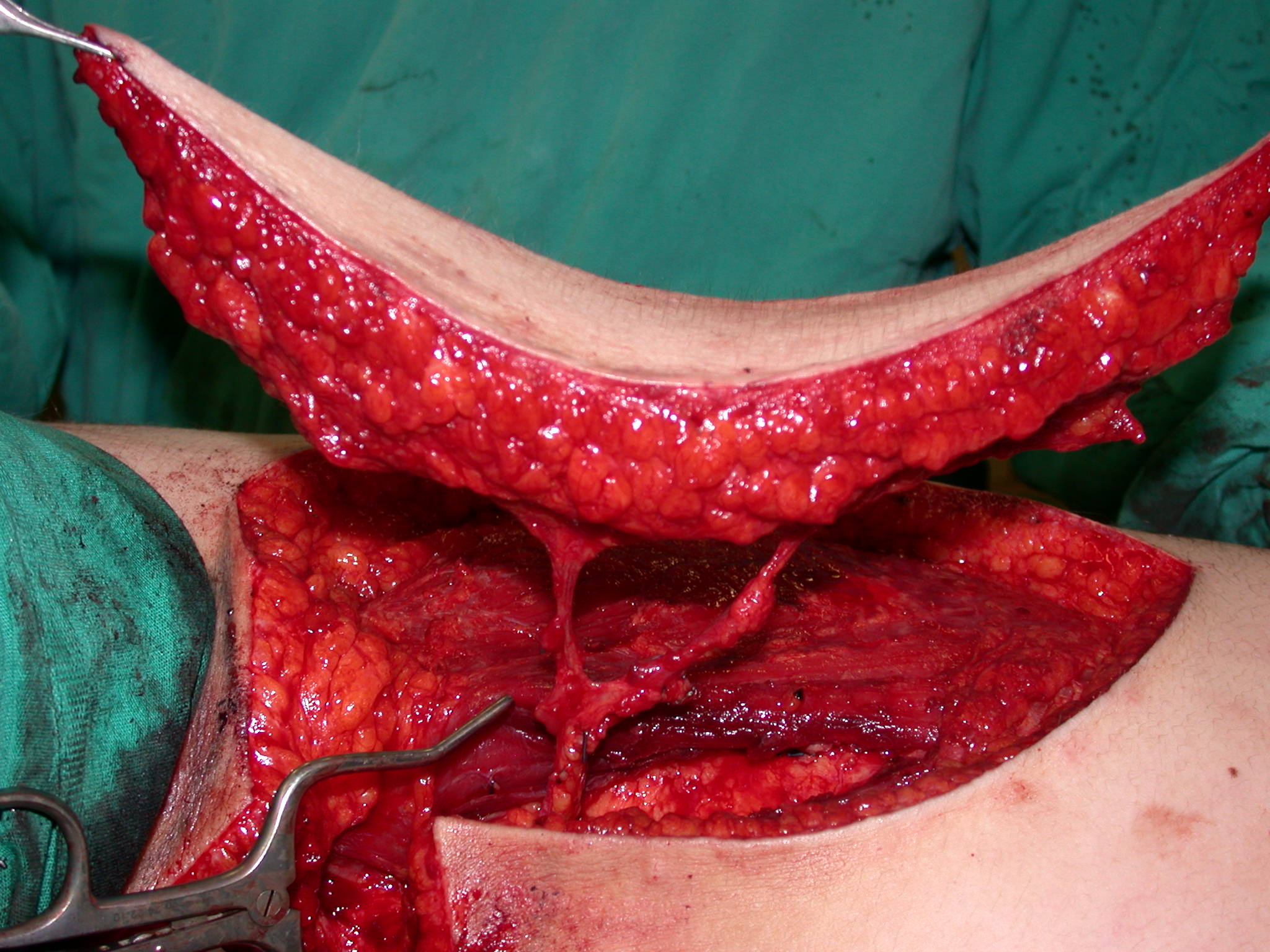
| Background: Axillary hidradenitis suppurativa is a chronic debilitating disease complicating with unpleasing fibrosis and scarring, which causes contracture and decreased mobility of the upper limb. Surgical removal of the involved area is the most effective treatment particularly among chronically affected patients. Patients and methods: Here we present the treatment of bilateral recurrent axillary hidradenitis suppurativa in three patients using 5 pedicled TAP flaps (Fig.1). The patients underwent two staged excision and reconstruction for each site at an interval of 8 weeks. All affected hair-bearing area was excised down to the axillary fascia and the remaining defects were covered with thoracodorsal artery perforator flaps (Fig.2). In one patient, a reliable perforator could not be found at one site and it was converted to a musculocutaneus pattern with minimal latissimus dorsi muscle sacrifice. Postoperatively, all patients received antibiotic treatment and immobilization of the arm. Results: There was only one surgical complication in terms of perforator rupture during the flap elevation, but the other perforator was sufficient for the flap survival. One patient required subsequent contour restoration of the flap. All flaps healed uneventfully and there was no recurrent disease or scar contracture within mean follow-up period of 10 months (Fig.3).The mean postoperative hospitalization was 6 days and no impairment of shoulder movement occurred in the early or late postoperative period. The aesthetic results of both the reconstructed area and the donor site have been satisfactory, subjectively and objectively. Conclusion: Reconstruction of the axillary defect remains a challange, especially in the extensive disease. Reconstruction of the mobile, three-dimensional axillary region with thoracodorsal artery perforator flap is preferable because of their excellent blood supply, reliability and the durability in addition to their excellent resemblance to the excised tissue. The disadvantage of the TAP flap is the need of meticulous pedicle dissection technique, especially for inexperienced surgeons. If the reliable perforator could not found, it is easy to convert the flap to a musculocutaneus pattern with minimal latissimus dorsi muscle sacrifice. This technique is suitable in the reconstruction of the excised recurrent obstinate large axillary hidradenitis suppurativa defects.
| ||
 |  |  |
| Figure 1 | Figure 2 | Figure 3 |
View Synopsis (.doc format, 268.0 kb)