
Sunday, October 8, 2006
10431
Three-dimensional Image Manipulation in Patients with Facial Skeletal Asymmetry: From Concepts to Surgical Practice
BACKGROUND
Recently there has been tremendous evolution both in the quality of three-dimensional computed tomography (3DCT) and in the sophistication of software for manipulating those images. While this technology has proven to be invaluable in diagnosis, there remains significant potential for its application in the operating room. At our center we recently have been using image manipulation software to plan facial contouring operations for young adult patients with facial asymmetry. Here we present our approach in using such software to plan corrective procedures in three patients. METHODS
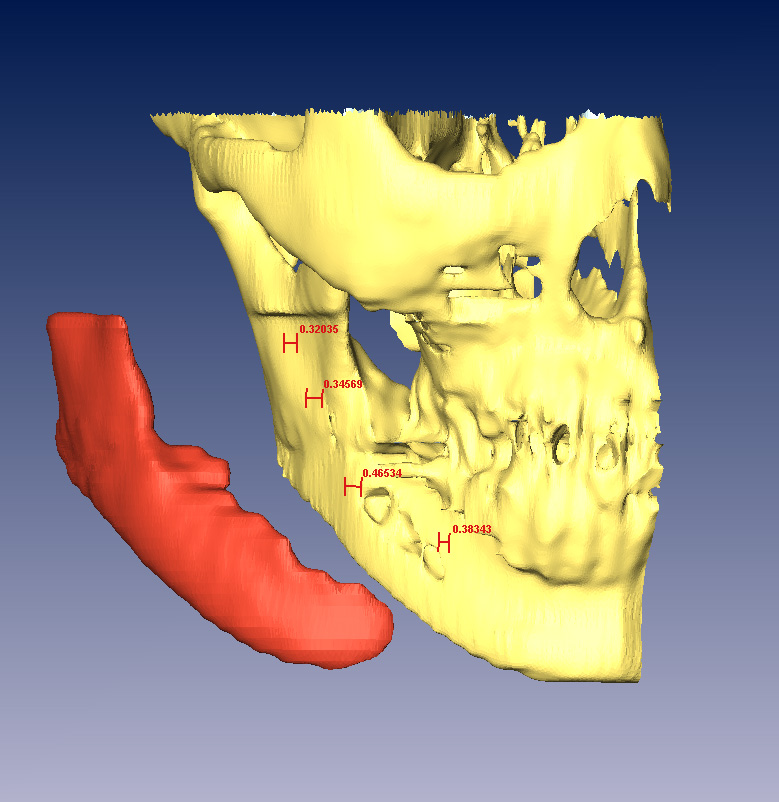
Three Taiwanese women of ages 21, 33, and 28 (patients 1, 2, and 3, respectively) presented to our clinic, each with the complaint of facial asymmetry. In patients 1 and 2, the asymmetry was developmental, affecting primarily the mandibular ramus and body ( ; all images refer to patient 2). Patient 3 had undergone previous cosmetic contouring of the zygomas, mandibular angles, and chin by another surgeon and now sought consultation for mandibular angle asymmetry and a disproportionately long lower face. For each patient a facial 3DCT was obtained and CT data was imported into Amira 3.1.1 software (Mercury Computer Systems Inc. San Diego, CA) to create a 3D skeletal model. A midline skeletal plane was constructed using the nasion, nasal septum, anterior nasal spine, and dental midline. The image was rotated posteriorly to assure that the most clinically applicable plane was chosen. Based on the patient and surgeon's subjective feeling of her most aesthetically favorable side, a mirror image was created of the corresponding computer-generated hemiskeleton. The actual and mirror images were compared through digital subtraction to determine the type and extent of contouring that would best achieve skeletal symmetry. This resulted in a 3D representation having specific dimensions (measured in millimeters) of the portion of skeleton to be augmented, or reduced (
; all images refer to patient 2). Patient 3 had undergone previous cosmetic contouring of the zygomas, mandibular angles, and chin by another surgeon and now sought consultation for mandibular angle asymmetry and a disproportionately long lower face. For each patient a facial 3DCT was obtained and CT data was imported into Amira 3.1.1 software (Mercury Computer Systems Inc. San Diego, CA) to create a 3D skeletal model. A midline skeletal plane was constructed using the nasion, nasal septum, anterior nasal spine, and dental midline. The image was rotated posteriorly to assure that the most clinically applicable plane was chosen. Based on the patient and surgeon's subjective feeling of her most aesthetically favorable side, a mirror image was created of the corresponding computer-generated hemiskeleton. The actual and mirror images were compared through digital subtraction to determine the type and extent of contouring that would best achieve skeletal symmetry. This resulted in a 3D representation having specific dimensions (measured in millimeters) of the portion of skeleton to be augmented, or reduced (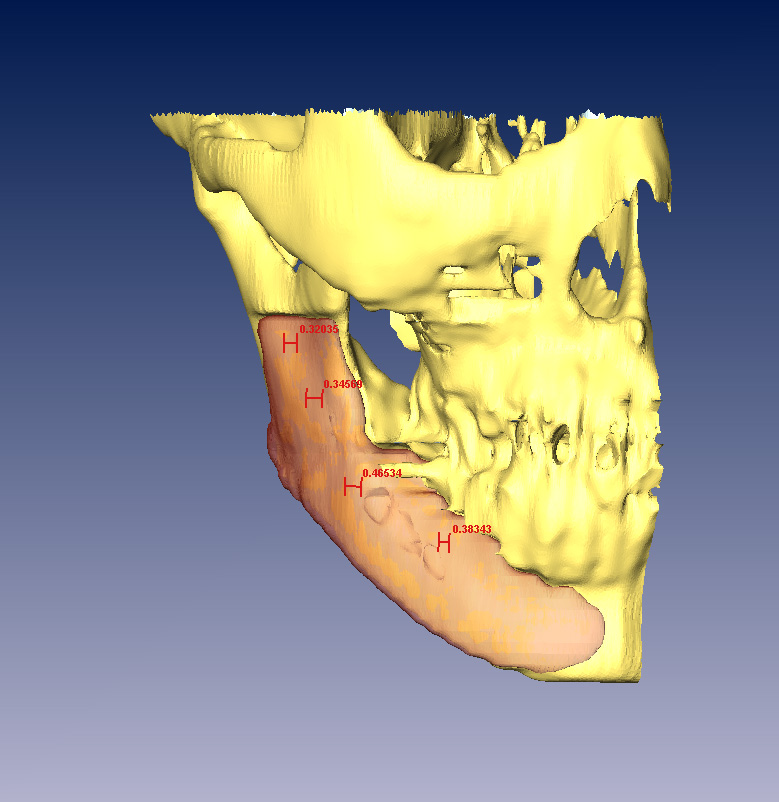 ,
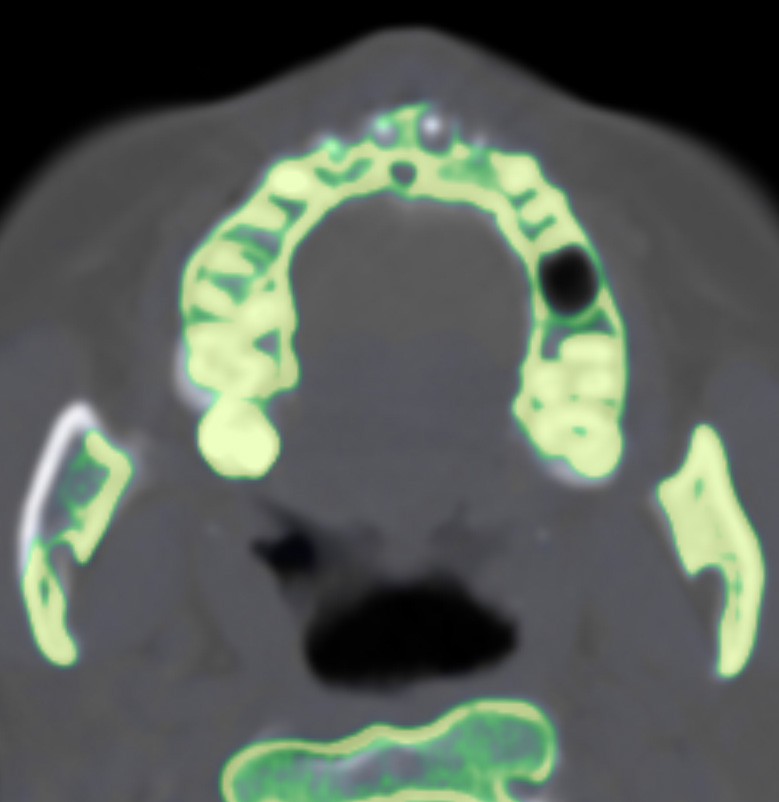
, ). The asymmetry was corrected through mandibular angle resection (patient 1) and burring of the outer cortex of the hemimandible to the extent and in a manner to achieve a bony resection having the morphology of the planned segment to be resected (patients 1, 2). Patient 3 underwent osseous shortening genioplasty and augmentation of the left mandibular angle with a Medpor prosthesis. The prosthesis was contoured intraoperatively to the form and dimensions calculated by our simulation. Postoperative CT scans were superimposed onto preoperative scans to determine accuracy of resection (
). The asymmetry was corrected through mandibular angle resection (patient 1) and burring of the outer cortex of the hemimandible to the extent and in a manner to achieve a bony resection having the morphology of the planned segment to be resected (patients 1, 2). Patient 3 underwent osseous shortening genioplasty and augmentation of the left mandibular angle with a Medpor prosthesis. The prosthesis was contoured intraoperatively to the form and dimensions calculated by our simulation. Postoperative CT scans were superimposed onto preoperative scans to determine accuracy of resection (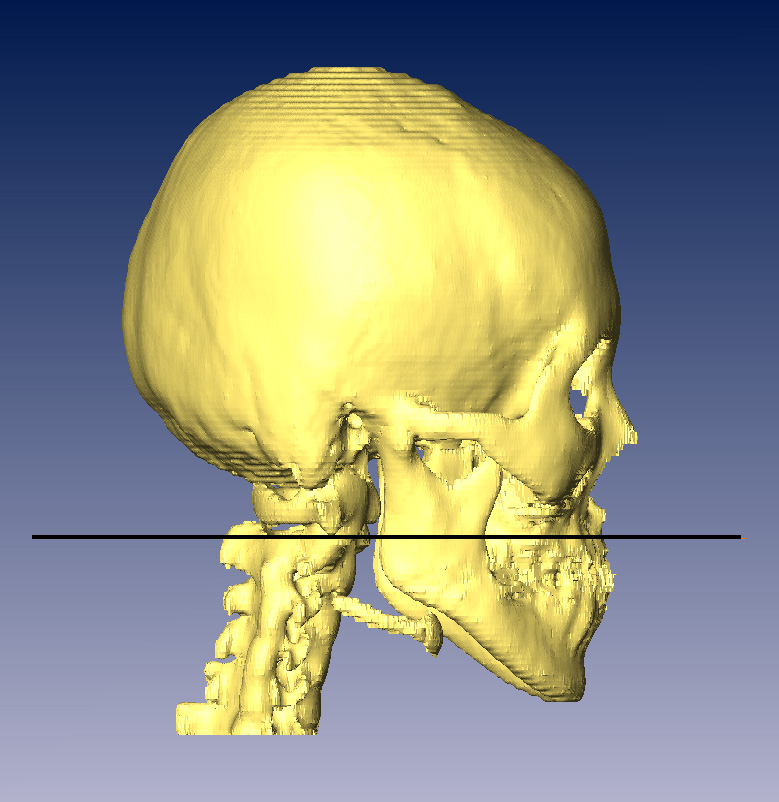 ,
, ). RESULTS
). RESULTS
Pre and postoperative CT superimposition revealed good correlation of the resected hemimandible with the planned area of resection. Each procedure was performed without complication and postoperatively each patient has demonstrated significant improvement in facial contour ( ). CONCLUSION
). CONCLUSION
The use of 3DCT combined with mirror imaging software has enabled a quantitative morphologic analysis of the deformity in this group of young adults with facial asymmetry. It has facilitated a surgical approach characterized by quantitative endpoints of recontouring. Our early experience is promising in that this relatively simple technique has afforded significant clinical improvement in this group of patients.
View Synopsis (.doc format, 1790.0 kb)