
Sunday, October 8, 2006
10741
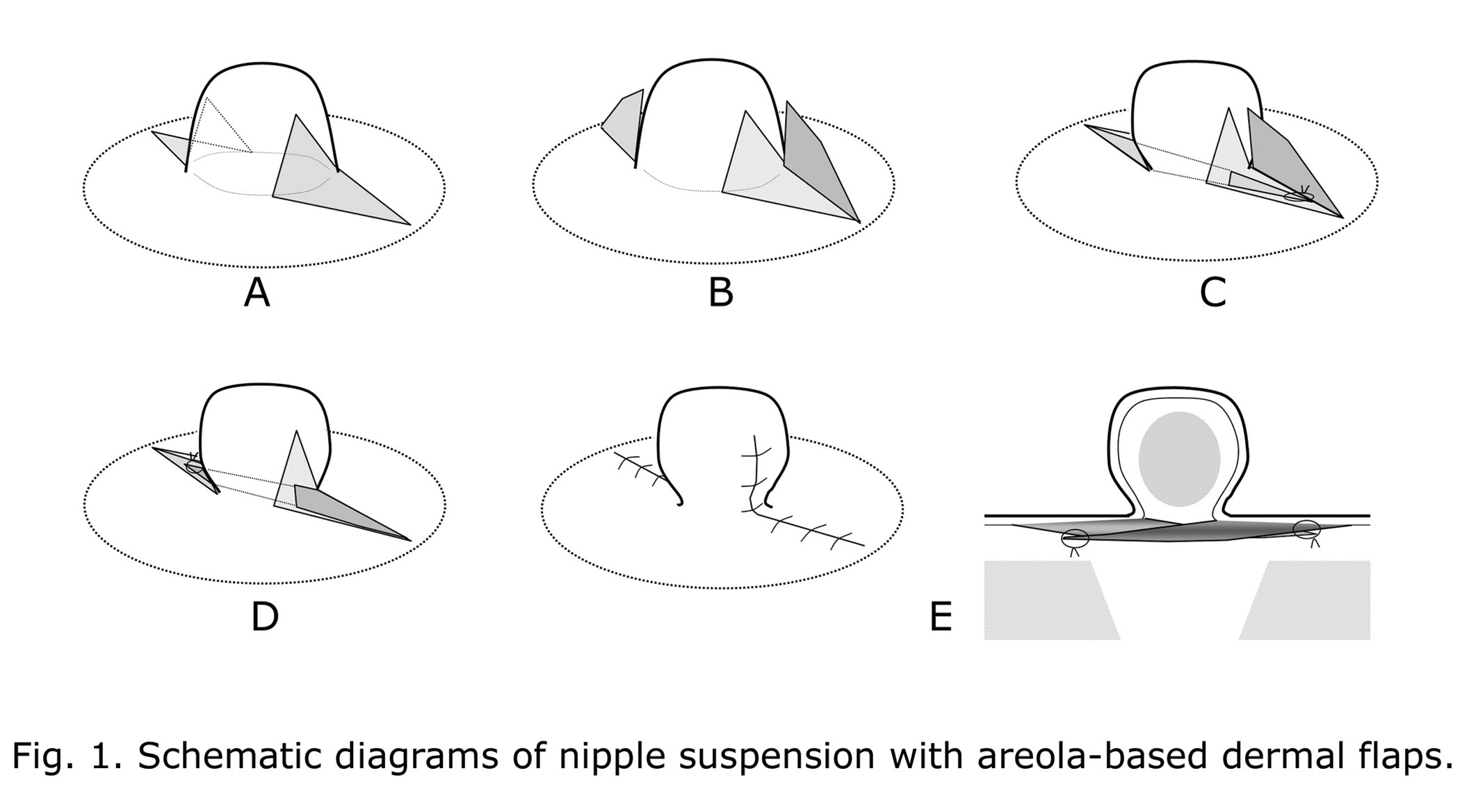
Correction of Inverted Nipple using Nipple Suspension with Areola-based Dermal Flaps
For correction of the moderate and severe inverted nipples, many surgeons have used triangular areolar dermal flap technique or its modifications with the concept of adding bulk or strut underneath the nipple. The base of these flaps is placed at the nipple neck. If the nipple neck is not reconstructed tightly, these nipple-based dermal flaps can be pulled down simultaneously with the nipple by scarring or retraction force. Thus these techniques have some risk of recurrence of inverted nipple, especially in the severe inverted nipple. If the bases of dermal flaps, as the fulcrums, are placed on the areola which is supported by the compact subcutaneous tissue and the mammary gland, these flaps may resist strongly against scarring or retraction force and may support the nipple more effectively. So I developed a strong nipple suspension method using areola-based dermal flaps for correction of moderate and severe inverted nipples. In moderate inverted nipples, two diamond-shaped quadrangles are marked horizontally at 3 and 9 o'clock position. In severe inverted nipples, four quadrangles are marked at 3, 6, 9 and 12 o'clock position. Dermal flaps are raised with a pedicle along one side of the areolar part of quadrangle. The tips of the nipple part of dermal flap are turned down through the tunnels and sutured at the opposite areolar dermis (Fig.1). Then the nipple is supported by two or four dermal flaps with each two rigid areolar fulcrums. The donor sites are closed with no nipple traction splinting. A donut dressing is only applied to avoid compression of the nipple. Of 28 nipples in 17 patients with moderate or severe inverted nipples, 19 nipples is moderate type and 9 is severe type. Patient age ranged from 21 to 39 years. Follow-up examinations (2 to 8 months) revealed no evidence of recurrence of inversion. There were no complications such as traction pain, infection, hematoma, permanent numbness, or skin necrosis. Most of cases (27 nipples) resulted in excellent projection, even in case of severe inversion after mastitis. In conclusion, areola-based dermal flap method has the concept of strong nipple suspension with two or four dermal flaps having the areolar fulcrums, and then allows correcting all types of the inverted nipple with preservation of the lactiferous ducts.
View Synopsis (.doc format, 262.0 kb)