
Monday, October 29, 2007 - 9:15 AM
13510
Extreme Distraction: What are the Practical Limits to the Amount of Mandible Dstraction that can be Achieved?
Background: Mandibular distraction has become the standard treatment for congential micrognathia. There is no clear consensus regarding practical limits of this procedure in terms of bony stability, adequate secondary growth, dysphagia, and need for secondary distraction.
Objective: To identify the practical limitations of external mandibular distraction in a severely micrognathic population.
Methods: A total of 46 patients have undergone "extreme" distraction, generating mandibular callus in excess of 50% of preoperative mandibular body or ramus length. Of these, the majority were Pierre Robin (n=23) patients. The remainder were Nager syndrome (n=7), Treacher Collins (n=7), OAVS (n=5) or rare syndromes. External "No-Vector" 2 pin distraction was used in all cases, with extreme overdistraction (35-40% sagittal overdistraction), planned relapse, and intentional generation of posterior open bite. All patients underwent MLB, 3dCT, cephalometric analysis, and repeat studies after surgery. Most underwent cine-MRI in cases of equivocal sleep study.
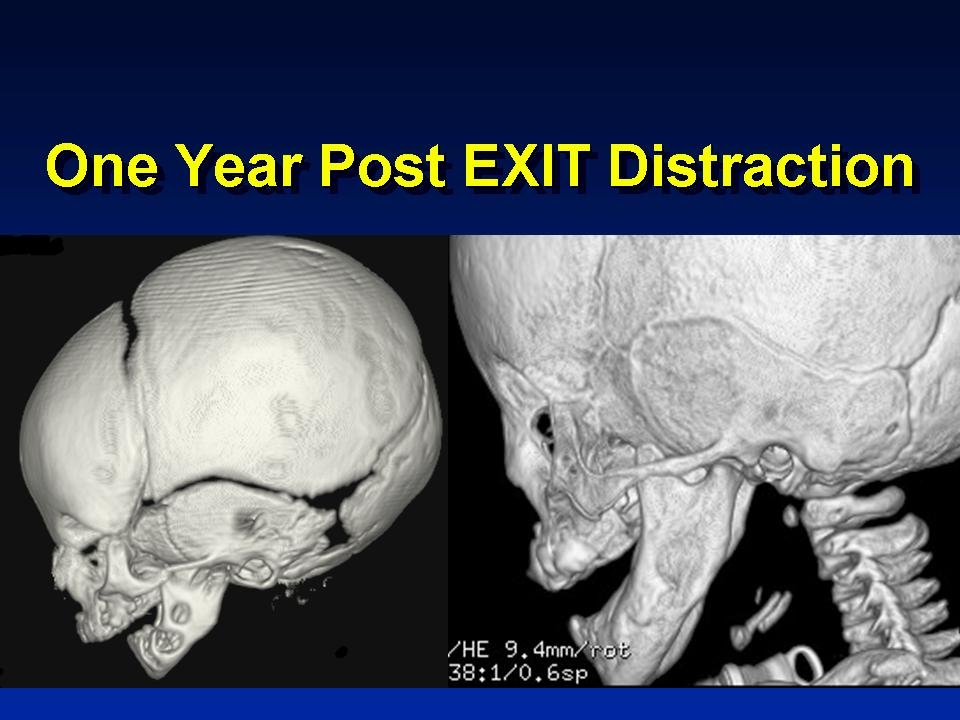
Results: The average extreme distraction case resulted in 33 mm of new regenerate in the neonatal group, 44 mm in the pediatric group, and 57 mm in the skeletally mature group. After planned relapse, these had reduced to 26, 34 and 46 mm respectively. There were 8 patients who subjectively reported diminished lower lip sensation. 4 had severe postoperative dysphagia, and in one patient with Moebius syndrome, reoperation with mandibular setback was needed to correct symptoms of VPI and dysphagia. Velopharyngeal dysfunction occurred in 5, and the remainder improved spontaneously. Redistraction was needed in a single patient within 18 months for poor growth and in another for incomplete airway correction at 5 months postoperatively. (Manske-Catel and profound Nager syndromes, respectively) In all OAVS patients, inadequate growth of the affected side will likely require redistraction in the mixed-dentition stage for slowly developing laterognathia. Stability of regenerate after planned collapse is superior to previously used methods in our hands, and there is no "waist" phenomenon with this technique.
Conclusion: There is no apparent functional limit to the amount of bone lengthening in the severely hypoplastic mandible. Rates up to 6 mm daily and overall distractions of up to 300% of initial mandibular size are achievable. Airway and soft tissue considerations must govern appropriate lengthening in this group. In our experience, this population should be approached with external distractors and minimal dissection for best results.
See more of Cranio/Maxillofacial/Head & Neck
Back to 2007am Complete Scientific Program