
Sunday, October 28, 2007
12676
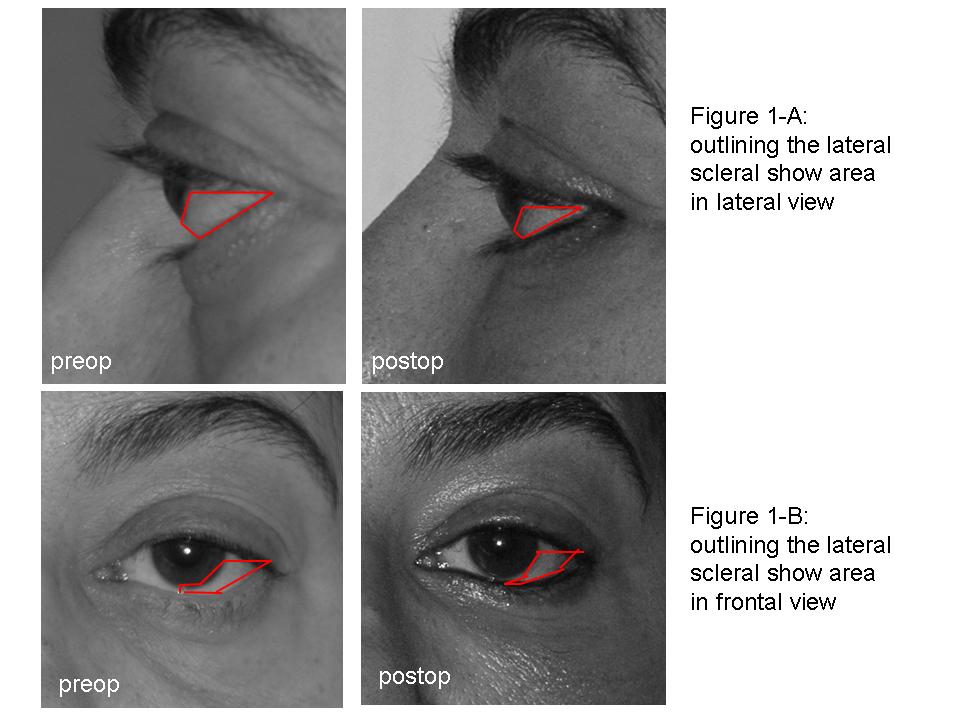
Volume Restoration of the Medial Tear Trough Deformity and Inferolateral Orbital Unit Decreases the Scleral Show
INTRODUCTION Increased scleral show is usually a result of lower eyelid laxity due to the aging process, iathrogenic lower eyelid midlamellar contraction, or proptosis of the eye globe producing an unaesthetic periorbital balance. We have been utilizing autologous adipose tissue for correction of the medial tear trough deformity and for volume restoration of the inferolateral periorbital unit. During the review process of the pre-operative and post-operative results of these patients, we have realized a significant decrease in lower eyelid scleral show for the frontal and lateral views, and a setback of the eye globe in the lateral views. These unplanned effects possibly contributed to the aesthetic improvement of the periorbital area seen in the post-operative views.
MATERIALS AND METHODS We decided to perform a retrospective study enrolling 20 patients who underwent inferior and lateral periorbital volume restoration with autologous adipose tissue transfer from inferior inner thigh SAL. The fat graft was injected in the subcutaneous preseptal plane, and the total volume ranged from 1.9 to 6.2 cc. Using preoperative and postoperative frontal and lateral views, straight and upper gaze, we analyzed the digital images. For the inferior scleral show component we measured the triangular scleral area in square pixels limited by a transverse line passing through the midpupil, the edge of the border of the inferolateral quadrant of the iris, and the border of the lower eyelid. To assess the degree of eye globe setback we measured the distance between the most projected midpupillary point and the anterior border of the lateral orbital rim in the straight gaze. The views were normalized for equal magnification and distance. We used parametric t student test for comparison between the scleral show areas and eyeglobe setback distances. We considered p < 0.05 for statistical significance.
RESULTS The area comparison for the scleral show revealed significant decrease postoperatively. The comparison of the distances described for the evaluation of proptosis also showed significant decrease in the postoperative views.
CONCLUSIONS The possible explanation for the discussed effects maybe hypothetically linked to the restoration of the support for anterior and inferior preseptal areas which were attenuated due to the descent and resorption of the supporting volume caused by gravity. The restoration of the preseptal compartment volume caudally at the level of the medial and inferior orbital rim delivers support inferoanteriorly to the preseptal stuctures in a cranial vector that secondarily pushes back the postseptal structures including the eye globe.
View Synopsis (.doc format, 145.0 kb)