
Sunday, October 28, 2007
12961
Progressive Tension Sutures in the Prevention of Post-abdominoplasty Seroma: A Prospective, Factorial and Randomized Clinical Trail
PROGRESSIVE TENSION SUTURES IN THE PREVENTION OF POST-ABDOMINOPLASTY SEROMA: A PROSPECTIVE, FACTORIAL AND RANDOMIZED TRAIL
á
á
Patricio Andrades MD, Arturo Prado MD, Stefan Danilla MD.
á
Division of Plastic Surgery, Department of Surgery, University of Chile School of Medicine
á
Background: Internal fixation techniques such as Progressive Tension Sutures (PTS) have arisen as a novel method to reduce post-abdominoplasty seroma. The purpose of this study is to evaluate the seroma reduction capabilities of PTS and compare them against the conventional use of drains.
Methods: Sixty female patients with a Matarasso type IV anterior abdominal wall deformity were randomized in four groups: Group 1 (control, without drains and without PTS); Group 2 (with PTS only); Group 3 (with drains only) and Group 4 (with PTS and drains). All the patients underwent a classic abdominoplasty and drains were left for 7 days in the corresponding groups. Clinical and Ultrasound (US) assessment were performed 2 weeks after the operation by masked evaluators. Needle aspiration volumes and non-seroma complications were recorded (Figure 1). After 6 months of follow-up aesthetic outcome were measured using subjective and objective systems by blinded surgeons.
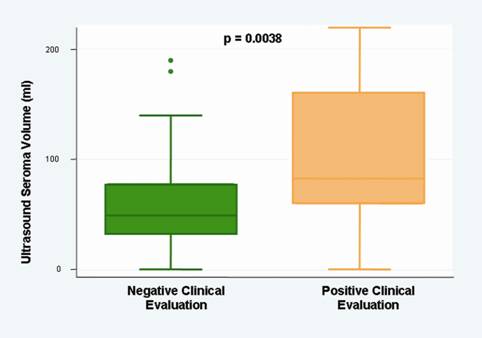
Results: Surgery time was, in average, 50 minutes longer in groups 2 and 4 where PTS were used (p<0.05). Drain outputs were higher in Group 3 than 4 where PTS were not used (p<0.05). The clinical and US seroma frequency was 35% and 90% respectively, without significant differences among the groups. Group 1 was the only one with large US seroma volumes, the rest had les than 65 ml. Control group had to be stopped at 10 patients because of larger seromas and increased amount of punctures needed for treatment, with no differences in the other groups (Table 1). Non-seroma complication occurred in 35% of the patients. Adequate relationship between US and Clinical Evaluation for the diagnosis of seroma was observed (p<0.05, Figure 2). There were no differences in relation to complication rate and aesthetic outcome after follow-up between the studied groups (Figure 3 and 4).
Conclusion: PTS increase the surgery time, reduce the drain outputs and have the same clinical and US seroma frequency than using drains only. The combination of both methods does not add any advantage but not using at least one of them increase complications and interventions. The mechanism of action of PTS could be the compartmentalization of the fluid collection under the flap facilitating absorption. áá TABLE I. Seroma analysis in the four studied groups.
á
á
|
á |
Group 1 Control N=10 |
Group 2 PTS N=15 |
Group 3 Drain N=15 |
Group 4 PTS+D N=15 |
Total N=55 |
p |
|
á |
á |
á |
á |
á |
á |
á |
|
Clinical Seroma |
50% |
33% |
33% |
27% |
35% |
N.S. |
|
á |
á |
á |
á |
á |
á |
á |
|
US Seroma |
100% |
87% |
87% |
93% |
90% |
N.S. |
|
á |
á |
á |
á |
á |
á |
á |
|
US Seroma Volume (ml.) |
155* Range 90-220 IQR 130-200 |
64 Range 0-90 IQR 36-79 |
45 Range 0-200 IQR 10-80 |
55 Range 0-110 IQR 40-70 |
80 Range 0-220 IQR 55-165 |
|
|
á |
á |
á |
á |
á |
á |
á |
|
Number of Compartments on US |
1 Range 1-2 IQR 1-1 |
3ć Range 0-4 IQR 2-3 |
1 Range 0-3 IQR 1-1 |
3ć Range 0-5 IQR 2-4 |
2 Range 0-5 IQR 1-4 |
0.001 |
|
á |
á |
á |
á |
á |
á |
á |
|
Surgery Time (hours) |
3.3 ▒ 0.3 |
4.2 ▒ 0.4 ć |
3.2 ▒ 0.6 |
4.1 ▒ 0.5 ć |
3.7 ▒ 0.5 |
<0.001 |
|
á |
á |
á |
á |
á |
á |
á |
|
Punctures Needed until negative |
9 * Range 7-13 IQR 8-10 |
1 Range 0-4 IQR 0-4 |
2 Range 0-4 IQR 1-3 |
1 Range 0-4 IQR 0-2 |
2 Range 0-13 IQR 1-4 |
<0.001 |
|
á |
á |
á |
á |
á |
á |
á |
|
*: Statistical differences for Group 1 only with no differences for the other studied groups ć: Significantly higher than Control and Drainage groups, but without differences among them. |
||||||
á
|
á |
á |
|
|
á |
á |
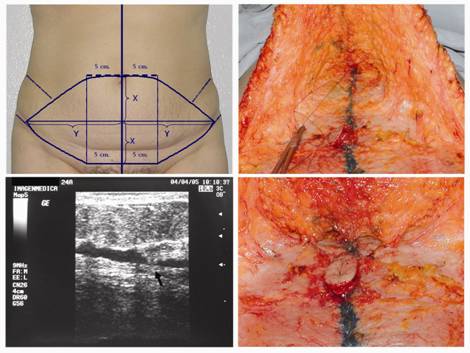
Figure 1: Markings, intraoperative PTS placement and US imaging showing PTS in place. á á
á |
áá
Figure 2: Relationship between Ultrasound and Clinical Evaluation for seroma diagnosis á
áá
|
á |
á |
|
|
á |
á |

á
|
á |
á |
|
|
á |
á |
