
Sunday, October 28, 2007
13027
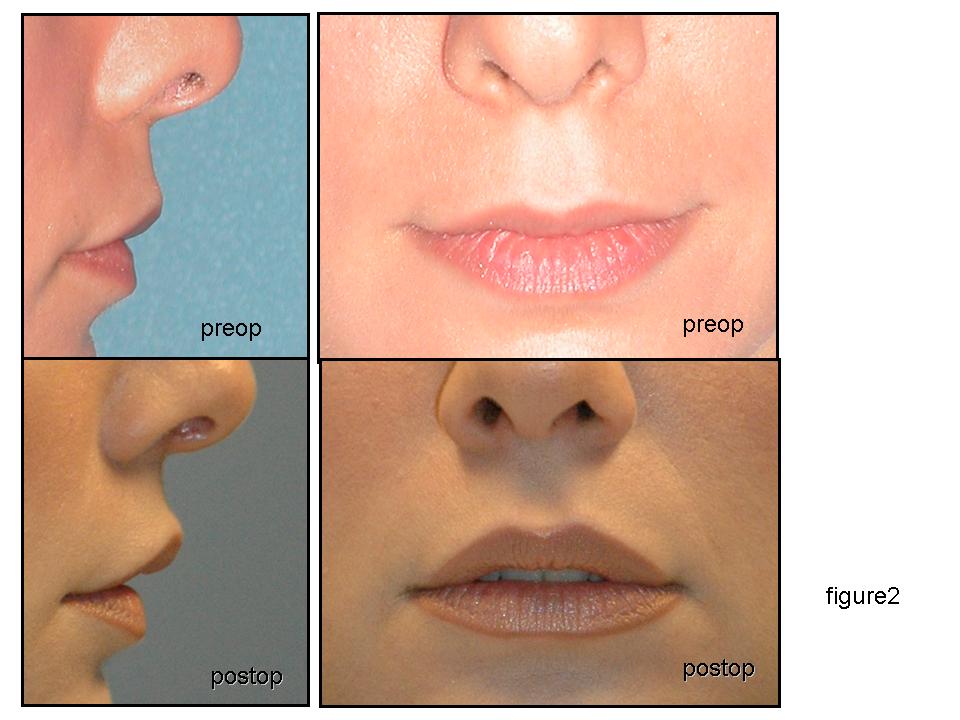
Suspension and Redrapping of the Free Columella - Lip Complex
INTRODUCTION The youthful and attractive look of the midface is determined by the distal nose to upper lip unit. For many years women have searched for a thick, voluminous upper vermillion thought of as the principal element of midface attractiveness. This has led to the development of many techniques to increase vermillion volume without addressing other midface components. However, the ideal configuration of the upper lip is that of a triangular shape with central elevation, yielding at least 2 – 3 mm of central incisive upper teeth exposure, which independently of other facial features gives freshness resembling the triangular mouth of an infant. These features accompanied by a short central upper lip, increased vermillion volume, adequate nose tip projection and columella length define the perfect components of an aesthetically pleasing midface. Correcting a long central upper lip, an acute nasolabial angle, a short columella and lack of tip projection would generally require many different procedures. Therefore the author suggests a simple technique which targets all the above mentioned midface components at the same time, as an additional maneuver during rhinoplasty or as an individual procedure.
MATERIALS AND METHODS 28 patients underwent the procedure proposed; 9 as an isolated in office procedure and 19 as an adjunct to a planned rhinoplasty. Patients where selected if they presented with the following features: long upper lip, lack of upper central incisive show or triangular upper lip figure with the mouth in the resting position, short columella or lack of nasal tip projection and acute nasolabial angle. Procedure: A transcolumellar, transfixion incision is performed and extended inferiorly in a horizontal plane 5 mm to each side of the columella. Blunt dissection is performed at the ANS and premaxilla releasing the depressor septi nasi muscle and the proximal border of the orbicularis oris muscle obtaining a free mobile columella – upper lip unit. The caudal septal cartilage is exposed free of perichondrium and nasal mucosa. Using 3-0 nylon two transverse thick bites are placed through the upper central margin of the orbicularis muscle from one nostril to the other within the extended incisions. These sutures are pulled in a cranial direction to be fixed at the caudal end of the septal cartilage in the reverse direction placing the knots one at each side of the septum to achieve symmetry. These circles of passant are tightened to a tolerable tension. The mucosa is closed by 5-0 plain fast absorbable sutures. Sometimes cephalic trim of the alar cartilages, and release of the dorsal skin unit are needed in conjunction when a rhinoplasty is not performed. Photographic evaluation and clinical observation where performed immediately after the procedure and at 3 month intervals.
RESULTS Photographic comparative pre and postoperative evaluation showed: a decrease in upper lip length with mean of 2 mm, a central upper lip elevation with 2 to 3 mm of upper incisive show, slight increase in vermillion thickness, increase in tip projection and increase in nasolabial angle. For the global midface assessment different observers including the patient agreed that the results following this procedure brought youthfulness, freshness and a very pleasing aesthetic result.
CONCLUSION This change in the configuration of the upper lip and distal nose provided by the redrapping and suspension of the free columella/lip unit is a simple procedure that addressed many features of the midface in one step obtaining an ideal aesthetic result.
View Synopsis (.doc format, 235.0 kb)