Friday, October 31, 2008
14082
Endoscopic Technique for Breast Tissue Expander Capsulotomy Using Carpal Tunnel Release Kit
Title
Endoscopic Technique for Breast Tissue Expander Capsulotomy Using Carpal Tunnel Release Kit
Introduction
During the process of tissue expansion in the breast, occasionally capsular contracture or implant malposition will occur.Ā Contracture may cause the implant to change position or become difficult to expand.Ā This usually requires operative intervention to release or remove the capsule to allow further expansion for breast reconstruction.Ā We present a minimally invasive technique for capsulotomy in the setting of breast tissue expander capsular contracture or malposition.
Methods
The Carpal Tunnel Syndrome Relief Kit (Linvatec, Largo, FL) designed for the Menon technique of endoscopic carpal tunnel release is used for the endoscopic capsulotomy.
We remove 120ml to 240ml of saline from the expander prior to incisions.Ā Short incisions are made at the lateral and medial ends of the previous mastectomy scar overlying the expander, each approximately 1.5cm long.Ā We dissect with electrocautery down to the capsule and enter it, taking care not to damage the expander.Ā The area of planned capsulotomy is bluntly dissected to create space between the capsule and expander.
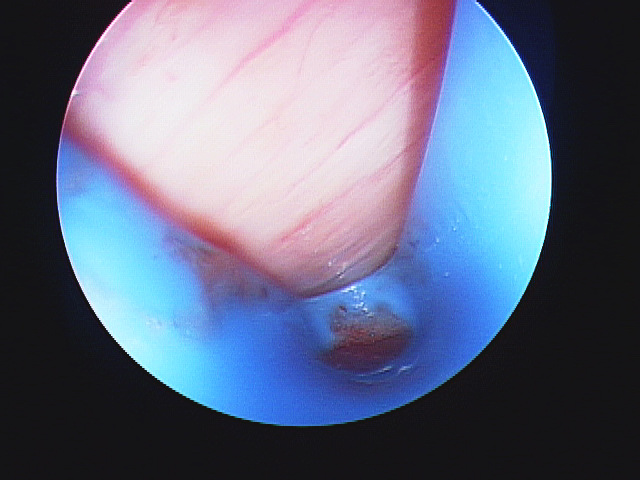
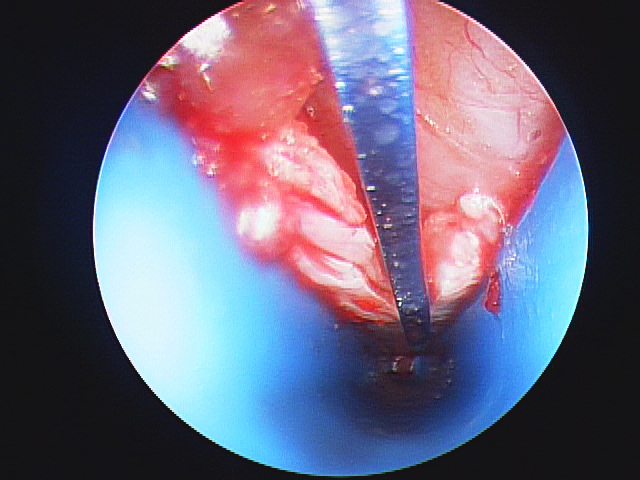
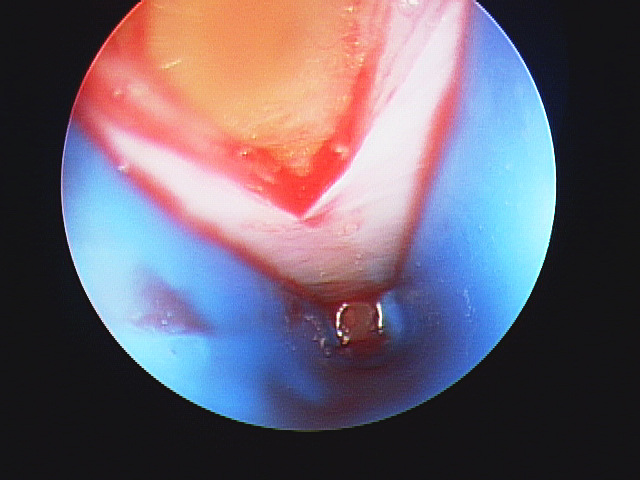
The D-shaped slotted cannula is then inserted under the capsule with a standard 30 degree angle 4mm arthroscope and the capsule is divided with the forward knife from the kit.Ā This is done under direct visualization with care to avoid damage to the expander.Ā To release the inferior capsule, we perform a V-shaped capsulotomy from both medial and lateral incisions.Ā

Blunt release of the capsule is performed and hemostasis is obtained.Ā The incisions are then closed in the standard fashion and saline is replaced in the expander.
Results
By this technique we are able to perform a capsulotomy with minimal incisions.Ā The capsule is released and the implant repositioned accordingly.
Discussion
The use of the endoscope in breast surgery has been reported in the literature for many years.Ā We present a new technique using the endoscopic forward knife in conjunction with the endoscope for release of the breast tissue expander capsule.Ā This allows for smaller incisions and potentially less discomfort after operative capsulotomy.Ā For those already comfortable with the endoscopic carpal tunnel release by Menon's technique, this can be a simple translation of technique to breast surgery.Ā The capsulotomy technique may potentially be extended to other indications for capsulotomy such as implant contracture or malposition.