Friday, October 31, 2008
14531
Latissimus Dorsi Chimeric Free Flap Reconstruction in Complicated Scalp and Calvarial Defects
Background: Adequate coverage of complex, composite scalp and cranial defects in previously radiated, infected or otherwise compromised tissue represents a challenge in reconstructive surgery. In order to provide wound closure with bony protection to the brain, improved cranial contour, and prevention or sealing of cerebrospinal fluid leaks, composite free tissue transfer is a reliable and safe option. We report our experience with five latissimus dorsi/rib intercostal perforator myo-osseo-cutaneous free flaps to reconstruct bony and soft tissue defects of the cranium and overlying scalp.
Ā
Methods: The surgical technique, design and outcome of the latissimus dorsi/rib intercostal perforator myo-osseo-cutaneous free flap reconstruction in five patients with cranial defects between 2003 and 2007 were retrospectively evaluated. Patient characteristics, defect size and underlying cause, reconstructive details and complications were analyzed.
Ā
Results: All patients (age 43 to 81) had complex cranial defects, mean size being 230cm2 (36-750cm2), two with cerebral spinal fluid (CSF) leak. Two patients had cranial defects due to malignancy (squamous cell carcinoma of the scalp, brain tumor with CSF leak), one patient had infiltrative cutaneous mucormycosis with osteomyelitis, one patient had infection of a failed cranioplasty after craniectomy for hemorrhagic stroke and one had continuous CSF leak after craniectomy for hemorrhagic stroke. Follow up ranges from 7-26 months. Complications included vascular compromise of one flap salvaged by vein graft, limited distal flap necrosis in three patients that was treated with local debridement and topical antimicrobial agents. No flap losses and no donor site complications were noted.
Ā
Conclusion: The latissimus dorsi chimeric free flap consisting of skin, muscle and vascularized rib based of the thoracodorsal artery can successfully cover large complex cranial defects, provide skeletal support, restore contour and significantly improve functional outcome with limited donor site morbidity.
Ā

Image1: Preoperative pictures showing large calvarial defect after failed cranioplasty with infection of cranial implant
Ā
Ā
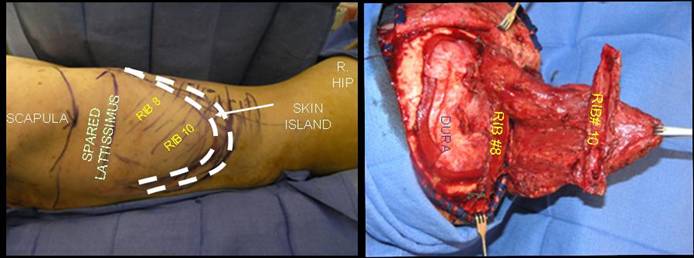
Image 2: Intraoperative markings for latissimus dorsi/rib intercostal perforator myo-osseo-cutaneous free flap and insetting of chimeric flap into cranial defect
Ā
Ā
Ā

Image 3: postoperative cranial reconstruction immediatly postoperative and at 3 month follow up