Friday, October 31, 2008
14564
Successful Recovering of Almost Amputated Dorso-Nasal Flap
In this case-report, an almost complete amputation of the nasal- dorsum, tip and right ala sub-units were successfully repositioned, recovering the original nasal shape.
CASE REPORT
A 19-year-old patient had a traumatic almost complete amputation of the nasal dorsum after fell down during the bath. The injury result in avulsion the dorsum, tip, and right ala sub-units. (Fig. 1) The flap was supplied by a small left ala pedicle, which presented an small epidermal laceration. The upper part of the mucosa and alar cartilages was connected with the avulsed cutaneous dermal tissue. The dorsal nasal upper cartilage including pericondrium was intact showing copious bleeding. A dermal pick with a 13x4.5 gauge needle over the dorsal surface of the flap reveled capilar bleeding even at its cranial part, although a cianosis nuance appeared when the flap was repositioned on its original bed. (Fig 2, 2-a) Local anesthesic (xilocaine) 5cc without epinephrine was infiltrated on the receptor site. The flap was then sutured over its native bed with 6-0 separated monofilament stitches, despite the discrepance between the pedicle pattern and flap size. The partial epidermal laceration over the left ala-the site of the pedicle was untouched. Finally, the anesthesiologist infiltrated the infra-orbital nerve bilaterally with 5cc bupivacaine without vasoconstrictor. (Fig. 3)
The patient was kept in warm room, in a 30o. elevated dorsal flexion position during five days. Every 4 hours the nurse cleaned the surgical site with warm saline solution and picked(stick) the cranial segment of the flap with a 13x4.5 needle to facilitate the venous drainage. Antibiotics(cephazolin) 1g TID, AAS 100mg BID and his regular anti-convulsivant drugs were continued.
At the fifth post-operative day the flap appeared with satisfactory nutrition and the patient was discharge to ambulatory follow-up. (Fig. 4) Two weeks later the nasal anatomy was restored, with total integration of the pseudo-avulsed flap and its sub-units. (Fig. 5, 6, 7)
DISCUSSION
Investigation about the facial angiossomes demonstrated the abundant nutrition around the neck, face, and the nose sub-units. Empiric experience along the time was reflected by the numerous nasal flap patterns with random or axial nutrition. In this case report the trauma energy was enough to almost amputated the dorso-nasal tissue. Even the thin left ala pedicle presented a linear cut comprising the epidermis. The lateral nasal artery branch of the angular , supplied the avulsed flap. (Fig. 8) The first thought of the surgical team was to complete the amputation and restore the lesion with the medio-frontalis flap. This idea was refuted, when we observed satisfactory bleeding after picking the flap with a 13x4.5 gauge needle. We just suture the flap over the native bed with 6-0 separated stitches. The anesthesic block of the infra-orbitalis nerve was intended to improve the vascular supply by simpathetic block of the region. Therefore, a cianosis was present at the end of the surgery because of the insufficient venous drenage. Probably, leches could be an alternative to improve the venous drainage, but this facility was not at hand in our practice. So, We tried to solve this issue keeping the patient in a warm room at a temperature around 28o.-30o.C. Every 4 hours the nurse picked the dermis with a 13x4,5 B-D® gauge needle over the cranial flap site distal the pedicle area. After that, she performed a smooth massage using cotton wetted with warm saline in order to facilitate the flap venous capilar bleeding drainage. One week salicilic acid 100mg BID with its anti-plaquetary effect, helped to improve the vascular turnover.
Finally, this case demonstrates incredible vascular pattern over the nasal tissue that can guide to possible flaps design considering the nose sub-units. It is also a witness of the surgical team integration and that even in the challenging events, we have to try with faith and talent.

Fig. 1

Fig. 2

Fig. 2-a

Fig. 3

Fig. 4

Fig. 5

Fig. 6

Fig. 7
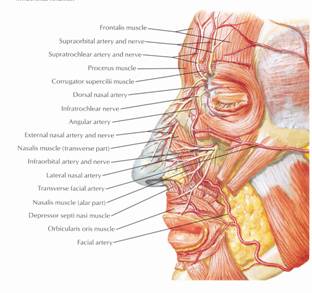
Fig. 8