Thursday, January 31, 2008
13725
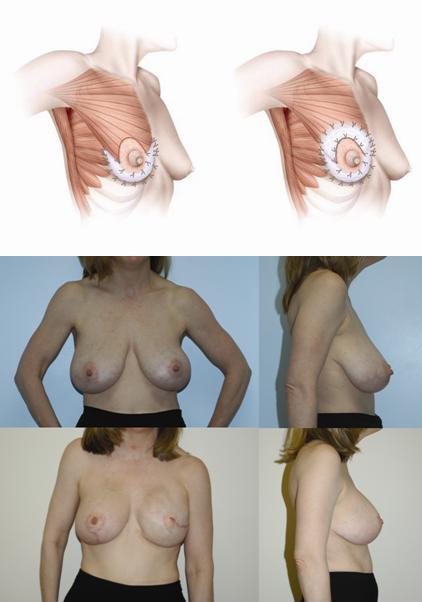
Improving Shape and Symmetry in Mastopexy with Autologous or Cadaveric Dermal Slings
Purpose: Mastopexy and reduction mammaplasty reshape breast parenchyma, elevate the nipple areolar complex, and restore a more youthful contour in women with ptotic breasts. However, results are often not sustained and recurrent ptosis is common. A plethora of reports over the last several years have attempted to address the shortcomings of this procedure, but none have been universally successful. In addition, it is difficult to match the shape of an implant breast reconstruction or an asymmetric constricted breast with current mastopexy techniques. The authors have been using internal autologous or cadaveric dermal slings to create conical breasts with long-term correction of ptosis for symmetry or rejuvenation. Methods: A retrospective review identified patients who had mastopexy or reduction mammaplasty/mastopexy with an internal dermal sling for circumferential support. Autologous dermal slings were created by deepithelialization of medial, superior, and lateral wings of the traditional Wise-pattern mastopexy. The lateral wing was secured to the lateral border of the pectoralis muscle and fascia thus recreating the normal lateral curvature of the breast. The medial and superior wings were draped around the breast in one or two layers and attached to the pectoralis fascia to create a circular breast mound. In cases of insufficient autologous skin, available autologous dermis was utilized and supplemented with cadaveric dermis (AlloDerm) for partial superior support. If autologous skin was poor in quality, AlloDerm was used for circumferential support. Results: Ten patients with an average age of 38yo (18-58) underwent unilateral mastopexy (3), unilateral reduction/mastopexy (1), bilateral mastopexy (5), or bilateral reduction/mastopexy (1) with an internal dermal sling. BMI ranged from 20-31 and all patients had grade 3 ptosis. Indications for mastopexy included a symmetry procedure after contralateral implant breast reconstruction (2), congenital asymmetry (2), and acquired ptosis with aging (3) or massive weight loss (3). Autologous dermis was used in five patients, and five patients were reconstructed with AlloDerm. Complications included one case of focal hypertrophic scarring. Breasts have maintained projection after a 6 month to 3 year follow-up. Two year follow-up after left mastectomy, implant reconstruction with an AlloDerm sling, and simultaneous right-sided mastopexy with a circumferential AlloDerm sling is shown in Figure 1 along with pre-operative photos for comparison and a technical diagram of our circumferential AlloDerm sling. Conclusion: Internal dermal slings improve and maintain breast projection in select patients undergoing mastopexy. A durable circumferential support system is created for the breast by securing autologous or cadaveric dermis to the immobile chest wall. The technique is quick, easy to learn, and reliable. An algorithm for choice of mastopexy technique is provided based on the quantity and quality of available skin.