Thursday, January 31, 2008
13866
Management of Contaminated Autografts in Plastic Surgery
Purpose: Contamination of autologous grafts unfortunately occurs in plastic surgery, but the literature provides no guidance for management of such incidents. A survey of plastic surgeons and a literature review were performed to create an algorithm for the management of contaminated autografts.
Materials/Methods: American Society of Aesthetic Plastic Surgery members were asked to complete an online survey that asked about the number and causes of graft contaminations experienced, how surgeons dealt with the problem, the clinical outcomes, and patient disclosure. In addition, a literature review was conducted to evaluate the best decontamination agent for each tissue type.
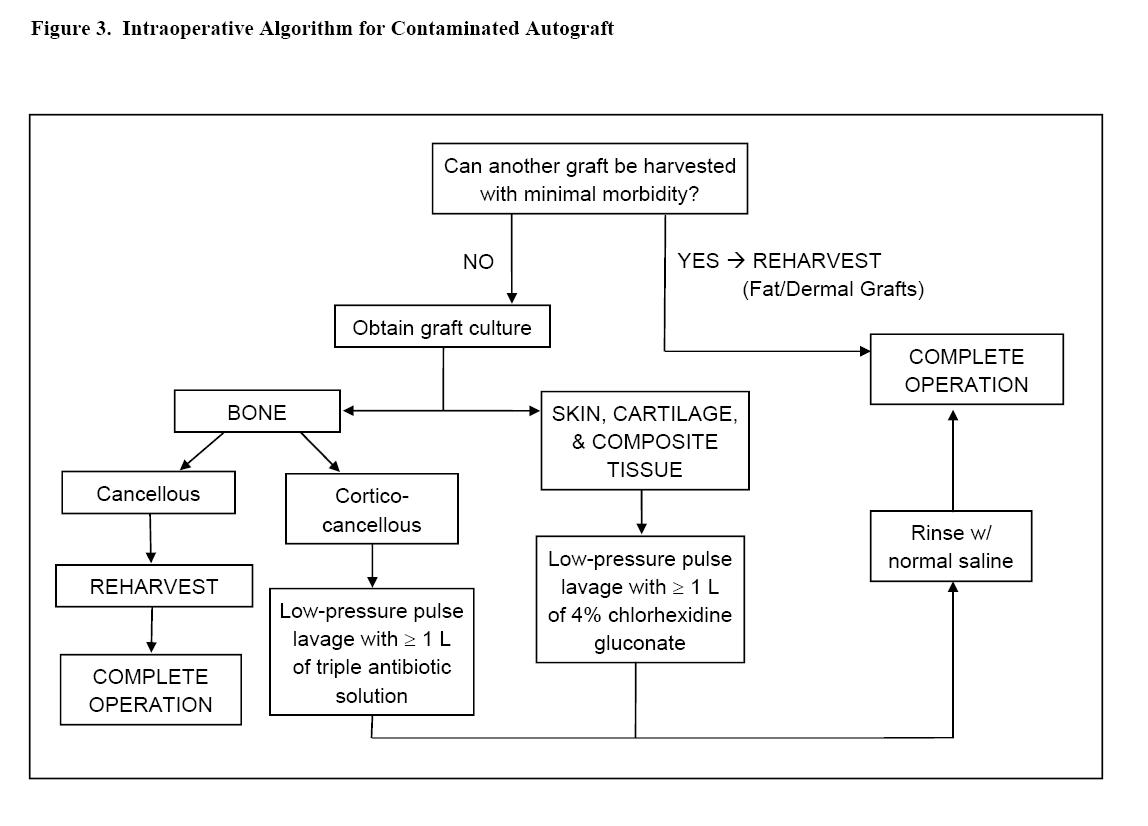
Results: Nineteen hundred surgeons were asked to participate in the survey, and 223 responded. Although the response rate of 12% was low, the survey does demonstrate that graft contamination occurs and the inconsistent method of decontamination. Of the respondents, 70% had experienced at least one graft contamination incident, with 26% experiencing four or more. The most frequently-reported reason for graft contamination was a graft falling on the floor (reported by 75%). Nearly two-thirds of the contaminated grafts related to craniofacial procedures. Ninety-four percent of grafts were managed with decontamination and completion of the operation. The most common method of decontamination was washing with povidone-iodine, but this practice is contrary to recommendations in the literature. Only three surgeons (1.9%) said a clinical infection developed following decontaminated graft use. Patients were not informed in 60% of graft contamination incidents. The survey results and review of the literature led to development of algorithms for the management of inadvertent graft contamination and patient disclosure. The algorithm recommends that skin, cartilage, and composite tissue grafts should be decontaminated with low pressure pulse lavage of 4% chlorrhexidine gluconate, while bone grafts should be decontaminated with triple antibiotic solution to prevent graft infection and minimize tissue damage. An algorithm on how to prevent such occurrences and a method with dealing with post-incident disclosures and perioperative management is also presented.
Conclusions: Although autologous grafts do become contaminated in plastic surgery, the overwhelming majority can be safely decontaminated and produce minimal or no clinical sequelae. The algorithms presented are intended to serve as guidelines for prevention of contamination events and for their management should they occur.