Thursday, January 15, 2009
14896
Internal Nasal Suspension for Correction of the Elderly Nose
PURPOSE
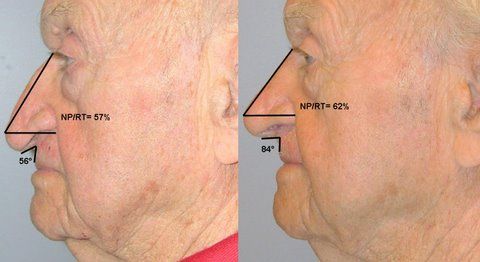
Suspension suture techniques have been implemented in a variety of plastic surgical scenarios that require the re-positioning of ptotic tissue. In this report, we describe an internal nasal suture suspension used to address the ptotic changes in an elderly nose. Our patient's deformity was characterized by a drooping nasal tip with associated marked acuity of the columellar-labial angle (56 degrees), partial coverage of the upper lip, and the impression of an elongated nasal dorsum. A highly effective, durable, cost-efficient, and safe technique is described here for the correction of this particular type of nasal deformity.
METHOD
An 87 year old, physically fit man requested correction of a long-standing, markedly under-projecting nasal tip. Under general anesthetic, a 28 mm transverse incision was placed within a deep procerus rhytid at the nasion. A subcutaneous pocket was then dissected along the dorsum to the nasal supra-tip region. 4-0 PDS on a 4cm straight needle was passed from the nasion incision, through the dorsal tunnel, and directed immediately cephalad to the junction of the right medial and lateral crura of right lower lateral cartilage. The right alar rim was everted and the needle partially delivered through the right nasal vestibular mucosa. A #11 blade was used to nick a 2 mm incision along the side of the needle. The needle was then fully retrieved from the right nostril and re-inserted through the 3 mm incision and passed across, within the plane between the septal cartilage and overlying domal cartilages, and then brought out partially through a complimentary location in the left nasal vestibule. A similar 3 mm incision was made along the side of the needle before retrieving it, passing it back into the incision, and directing it up and out through the nasion incision. The suture was then secured to periosteum under the cephalad edge of the nasion wound, and incremental tension applied until the desired nasal tip elevation and rotation was achieved. Video and still photography of the procedure were captured for illustrative purposes.
RESULTS
At 6 weeks and 6 months postoperatively there is excellent re-positioning of the nasal tip and associated widening of the columellar-labial angle to 84 degrees. Recovery was brisk no analgesia or ecchymosis – felt normal by POD2 The patient is very satisfied with his nasal appearance following this technique.
CONCLUSION
This case report describes a safe, highly effective, durable, and cost-efficient technique for management of the severely ptotic, under-projecting nasal tip, most commonly seen in the elderly patient seeking rhinoplasty. By avoiding the extensive dissection and tissue manipulation of either the open or closed rhinoplasty approach, this technique will be found to reduce the risk of associated ecchymosis, edema and pain, thereby shortening the recovery period. A highlight of this technique is the expectation for a reduction in operative time and the likelihood of being able to routinely perform this under local anesthetic.