
Thursday, January 15, 2009
14938
Use of the Vascularized Medial Femoral Condyle Periosteal Bone Flap for Repair of a Large Palatal Fistula
PURPOSE: The vascularized medial femoral condyle periosteal bone flap is a recently described free tissue transfer that has found its primary application in the treatment of upper extremity bony nonunions.Ā The advantagesĀof this application include versatility of size and shape of the flap, and highly osteogenic properties resulting from inclusion of cancellous, cortical, and periosteal components.Ā To date, this flap has not been utilized for the purpose of reconstruction of bony defects of the hard palate.Ā Treatment of large palatal fistulas is a challenging undertaking fraught with high rates of recurrence, and challenges in selection of adequate local or distant donor sites.Ā Free tissue transfer is performed when local options have been exhausted, with the radial forearm fasciocutaneous flap being most frequently selected for reconstruction.Ā The radial forearm flap, however, provides only soft tissue which may be inadequate to support the bony platform of the palate, and results in a significant donor site defect.Ā The purpose of this caseĀwas to utilize the vascularized medial femoral condyle periosteal bone flap for the novel indication of reconstruction of a large palatal defect.
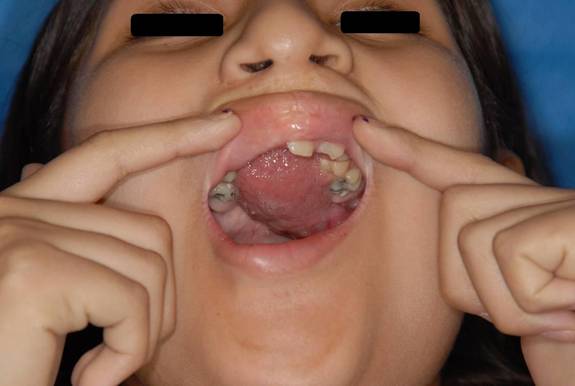
METHOD: This is a case of an 11 year old female with a history of bilateral cleft lip and palate who developed a large oronasal fistula with significant impact on speech.Ā After several attempts at reconstruction with local tissue failed, she was referred for free tissue transfer reconstruction.Ā The defect measured 2x3cm, and involved the hard palate without involvement of the soft palate.Ā To accomplish optimal reconstruction of both bony and soft tissue elements, and to minimize donor site morbidity, the medial femoral condyle periosteal bone flap was selected.Ā This flap has the advantage of providing composite tissue that is easily tailored to size, has a long pedicle, and results in minimal donor site morbidity and no disruption of growth.Ā The flap was secured circumferentially to mucoperiosteal flaps, and the vascular pedicle was tunneled through the lateral pharynx through the buccal soft tissues, reaching the facial vessels without difficulty.Ā

RESULTS: The flap healed well into position, and improvement of speech was immediate.Ā The donor site healed well without any complications, and resulted in no functional deficits.
CONCLUSION: To date, this flap has not been utilized for the purpose of reconstruction of palatal defects.Ā Because of its ease of harvest, versatile configuration and low donor site morbidity, the medial femoral condyle periosteal bone flap is an excellent option for composite reconstruction of large palatal defects.