
Saturday, October 2, 2010
17355
The Changing of Upper Lip Height and Nostril Floor After Grafting Bone in the Unilateral Cleft Lip and Alveolus Patients
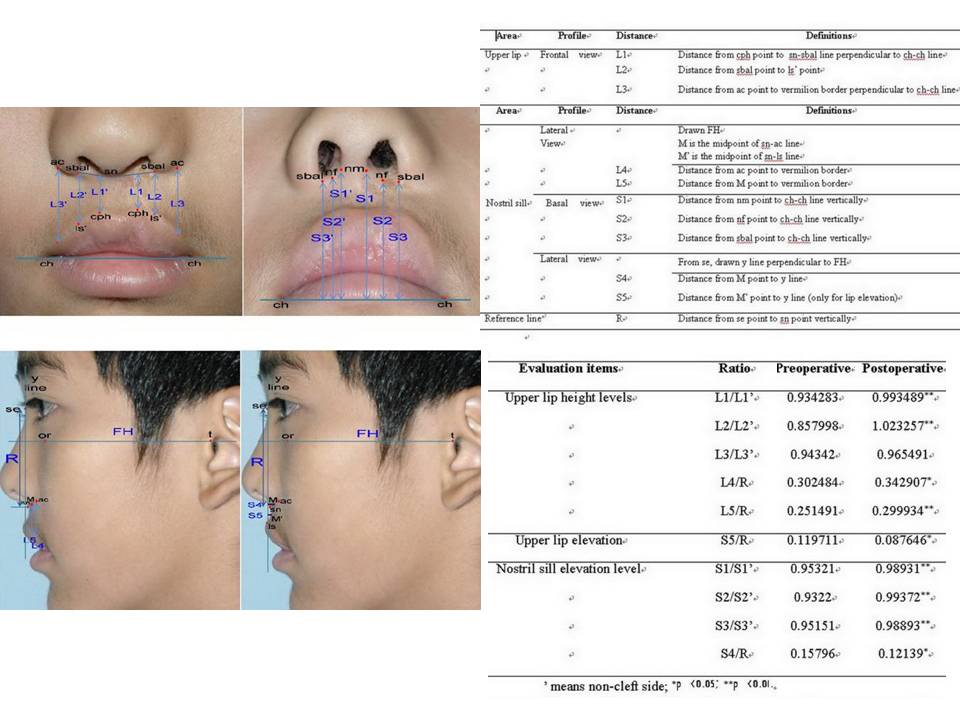
BACKGROUND & PURPOSE: Alveolar bone graft is performed to close the fistula, stabilize the maxillary arch, support root of teeth adjacent to the cleft and support prosthesis. After bone grafting, the upper lip and nostril sill on the cleft side will be changed. However there were rare reports about soft tissue change after alveolar bone grafting. The purpose of our study is to evaluate the change of upper lip height and elevation of nostril sill after alveolar bone grafting in UCLA patients by photogrammetry. METHODS: Fourteen UCLA patients who had been operated with iliac bone graft are surveyed by photogrammetry. The follow up periods are from one to two years. Preoperative and postoperative photography are taken including frontal view, base view and lateral view. For the evaluation, we made 5 distances (L1, L2, L3, L4, L5) for the upper lip height, 1 distance (S5) to evaluate the upper lip elevation and 4 distances (S1, S2, S3, S4) for the nostril sill elevation. The landmarks and distances are defined as figure 1 and table 1. After that, we calculate the ratio of cleft side to non cleft side at each distance as table 2. Finally, we compare the preoperative ratio with postoperative ratio using SPSS (Statistical Package for the Social Sciences) statistic software. RESULTS: Mean of each distance ratio is presented as table 2. For upper lip height on frontal view, preoperative ratio of L1/L1(non cleft side) and L2/L2(non cleft side) increased compared to postoperative ratio significantly (p< 0.01). Although preoperative ratio of L3/L3(non cleft side) increased compared to postoperative ratio, that is not significant. For upper lip height on lateral view, preoperative ratio of L4/R and L5/R increased compared to postoperative ratio significantly (p< 0.05, p< 0.01). Accessing the upper lip elevation, preoperative ratio of S5/R decreased compared to postoperative ratio significantly (p< 0.05). It means the upper lip was elevated postoperatively. For nostril sill elevation on basal view, preoperative ratio of S1/S1(non cleft side), S2/S2(non cleft side) and S3/S3(non cleft side) increased compared to postoperative ratio significantly (p< 0.01). For nostril sill elevation on lateral view, preoperative ratio of S4/R decreased compared to postoperative ratio significantly (p< 0.05). It means the nostril sill was elevated postoperatively. CONCLUSIONS: According to our study, upper lip height was increased and upper lip and nostril sill was elevated significantly after alveolar bone grafting. Although we can easily imagine the elevation of nostril sill after alveolar bone grafting, we can not easily imagine that upper lip is lengthened. Therefore our study is meaningful. MAIN OBJECTIVES OF PRESENTATION: Main objective of presentation is to announce that upper lip height was increased and upper lip and nostril sill was elevated significantly after alveolar bone grafting.
See more of Cranio/Maxillofacial/Head and Neck Paper (5 mins)
Back to 2010am Complete Scientific Program