Sunday, October 3, 2010
17641
Tertiary Plus Rhinoplasty: Recreating Deep Structural Subunits for Optimal Aesthetic Outcomes
The multiply operated nose, the severely traumatized nose and the cocaine nose have many similarities that challenge the aesthetic and reconstructive surgeon. Findings include shortened nasal length, lack of tip projection and severe scarring with limited extensibility and mucosa. We present a series of these challenging patients in which we apply a technique based on recreating the structural subunits of the nose and restoring an aesthetic nasal index.
Materials and Methods
All patients are managed in a closed manner with bilateral rim incisions. After complete liberation of the native cartilaginous structures from the scar and cutaneous cover, dissection continues to allow establishment of appropriate tissue envelope length. All previous grafts and foreign bodies are removed as necessary. Costal cartilage is harvested and two grafts are designed. The first graft recreates the deep structural subunit that corresponds to the skin subunits of the columella, soft triangles and tip. This graft takes the form of a short pyramid with an isosceles triangle as its base. The equal sides of the base triangle correspond to the distance from anterior nasal spine to the light reflex on each side of the tip(16-20mm). The third side is the width of the tip(8-10mm). The superior face of this pyramidal graft recreates the tip proper. A second graft re-establishes nasal length by coursing from radix to the posterior surface of the pyramidal graft. The step-off between this graft and the projetion of the pyramidal graft is 4mm in patients with thin skin and 8mm in patients with thick skin. A third gratft spanning between the upper lateral cartilages is added only when the internal nasal valve is compromised. Once grafting is completed a periosteal and galeal graft is harvested from the parietal scalp. This graft is draped over the entire construct to relieve the scarred appearance of the nasal skin.
Experience
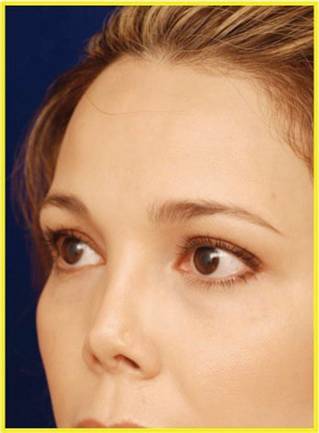
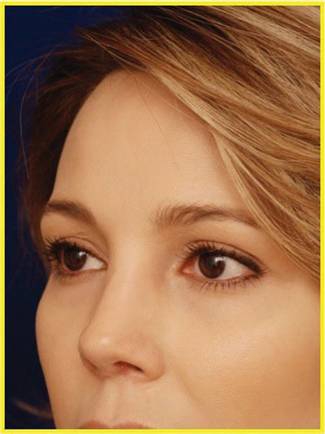
We have treated 20 patients 21-42 years old (mean 31) over the past decade with this technique. Each patient had between four and fourteen previous rhinoplasties. All patients were treated with the above described technique. We present 2-8 (mean 4) year follow up for each patient demonstrating restoration of an aesthetic nasal index and normal tip morphology. We have also corrected the scarred contour of the dorsal nasal skin with our periosteal-galeal grafting.
Conclusions
Using a technique that aims at restoring two deep structural subunits and blending soft tissue contour we are able restore a normal aesthetic appearing nose in this extremely challenging patient sub-population. We find a simplified two-subunit system for the deep structure of the nose recreates all cutaneous subunits and is advantageous to more complex frameworks. Secondarily these grafts are thick and structurally robust, thus resist the unique demands of the scarred inelastic soft tissue envelope in this patient subpopulation.