
Monday, October 4, 2010
17836
Pediatric Traumatic and Obstetrical Brachial Plexus Palsy: Triceps to Axillary Nerve Transfers to Restore Shoulder Abduction
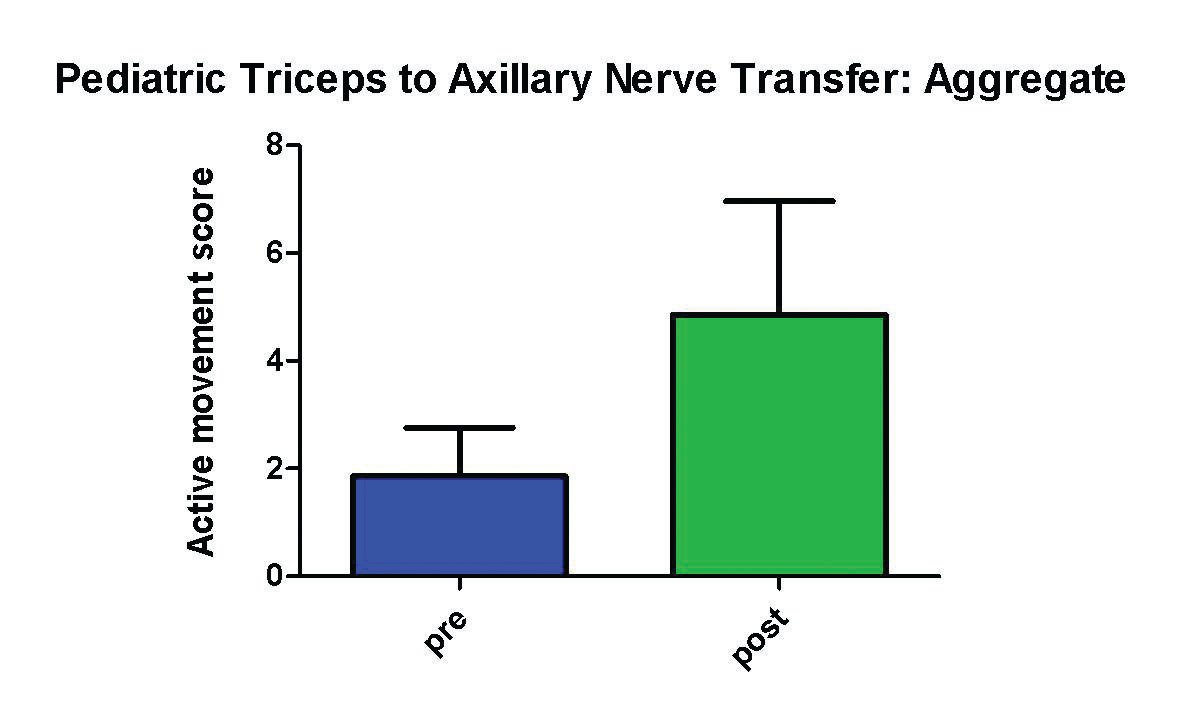
Purpose: Obstetrical and pediatric traumatic brachial plexus injuries produce substantial morbidity. In the case of upper plexus lesions, shoulder abduction is often difficult to restore. Transfer of the triceps branch of the radial nerve to the axillary nerve has been shown to be effective in adult populations in improving shoulder abduction. Data in the paediatric population is lacking. We sought to determine the utility and limitations of this transfer in this population. We present a series of seven patients in which this nerve transfer was used in children. Methods: Seven patients (age at presentation: 3 days to 14 yrs) underwent transfer of one or two triceps nerves to the motor branches of the axillary nerve. Pre- and postoperative scores were obtained using the AMS (Active Movement Scale, Clarke HM, Curtis CG. Hand Clin. 1995 Nov;11(4):563-80) and compared for obstetrical and traumatic cases. The effect on elbow extension was also assessed. Results: In aggregate, this transfer was able to generate antigravity shoulder abduction (AMS 5+, p < 0.05) in this series. Obstetrical cases, when treated before age 1 yr, were able to obtain antigravity shoulder abduction (AMS 5+, p < 0.05), in contrast to the late-presenting or salvage cases, which fared worse. Traumatic cases obtained antigravity shoulder abduction (AMS 6+, p < 0.05). There was no elbow extension deficit following transfer (pre- and postoperative AMS 7). Conclusions: In carefully selected cases, this transfer may be a useful adjunct in treatment of pediatric brachial plexus or axillary nerve injury.
See more of Hand & Upper Extremity (5 mins)
Back to 2010am Complete Scientific Program