
Monday, October 4, 2010
17920
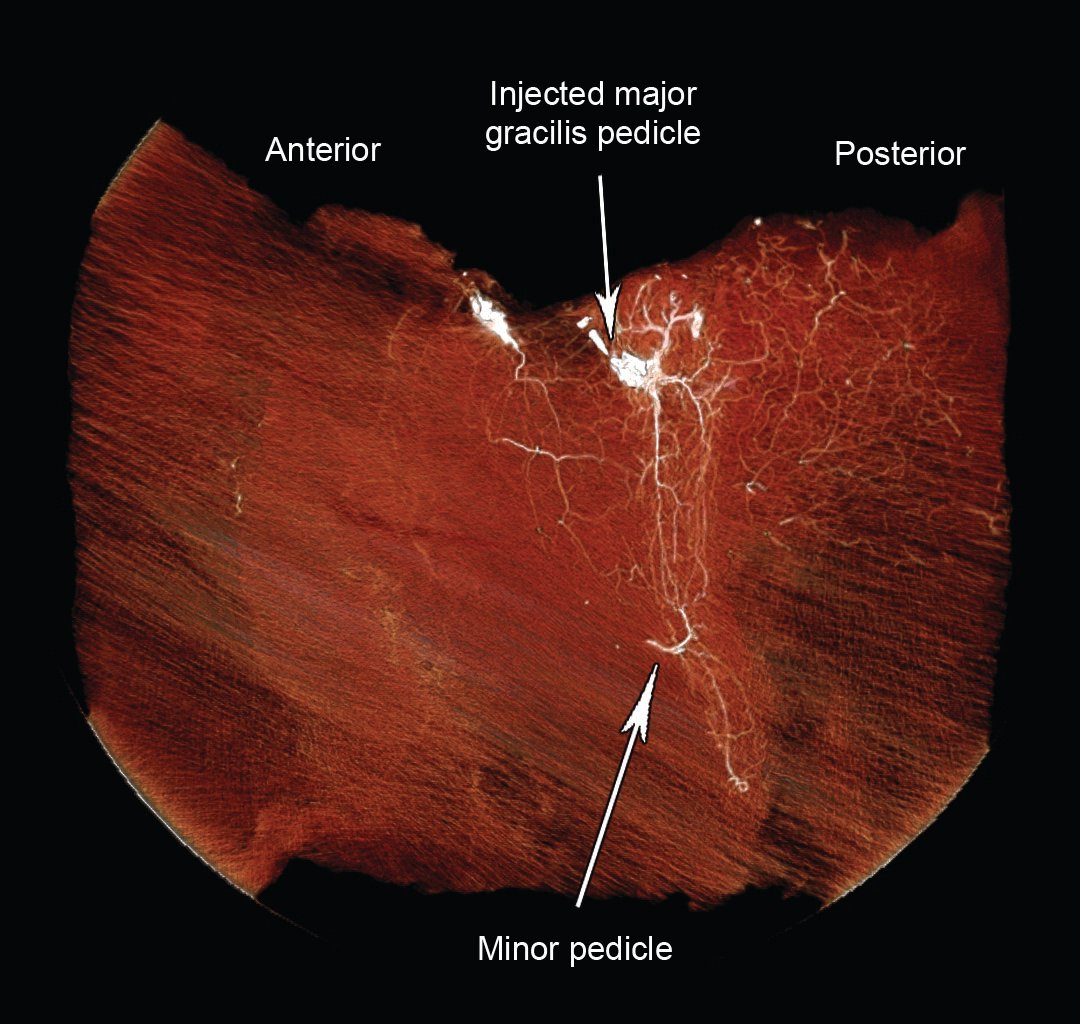
The Extended Transverse Musculocutaneous Gracilis (TMG) Flap: 3D CT Angiography and Clinical Series
Background: The transverse musculocutaneous gracilis (TMG) flap has been utilized in autologous breast reconstruction, but disadvantages include a small volume, compared to abdominal-based flaps. The vascular territory of this flap is investigated, with the possibility of extending its dimensions. We present two types of modifications to increase the bulk of TMG flaps, along with a case series for each modification. Methods: Ten circumferential thigh adipo-cutaneous flaps attached to the gracilis muscle were harvested from adult cadavers. The major pedicles were injected with contrast and subjected to 3D CT scanning. Images were viewed and the vascular territories measured. Flaps were then incised to include only tissue that was perfused with contrast, and measured for weight and volume. Twelve patients requiring autologous breast reconstruction between May 2009 and April 2010 were managed with TMG flaps which were modified with either a horizontal or vertical extension. Results: 3D images from contrast injection of the major pedicle showed a cutaneous vascular territory that extended more posteriorly than anteriorly, and had a vertical component. Tissue perfused with contrast had a mean weight of 573g and volume of 617ml. All (n=12) but two patients required bilateral breast reconstruction, thus giving 22 flaps in total. There were 6 patients with 10 Horizontal Extension TMG flaps, and 6 patients with 12 Vertical Extension TMG flaps. There were two cases of partial flap necrosis, two cases of fat necrosis, one case of donor site seroma and two donor site wound dehiscence. Conclusion: The dimensions of a TMG flap can be increased, both horizontally (supero-posterior thigh) and vertically. The extended portion can be harvested either by undermining the skin inferior to the lower transverse skin incision (horizontal extension), or by raising vertical skin extension, to harvest even more tissue from the medial thigh.
See more of Hand & Upper Extremity (5 mins)
Back to 2010am Complete Scientific Program