Saturday, October 2, 2010
18197
Creating a Virtual Surgical Atlas of Craniofacial Procedures. Surgical Animations
Background – Craniofacial surgery involves a mastery of the 3-dimensional anatomy of the face. The relative rarity of craniofacial malformations combined with the use of access incisions remote from the surgical area can make this type of surgery difficult to teach and learn. In order to augment the intra-operative learning experience for surgical trainees and to provide a resource for practicing craniofacial surgeons to review uncommonly performed procedures prior to entering the operating room, a series of 3-dimensional animations of the most common craniofacial procedures were created. This is the first virtual atlas of craniofacial surgical procedures.
Methods – Previously created, 3-dimensional digital models of the normal and pathologic craniofacial anatomy were used to create digital animations of craniofacial surgical procedures using Maya 8.5 (Autodesk, San Rafael, CA). These models contained detailed reproductions of the craniofacial skeleton, all overlying soft tissue elements as well as real-life textures of all tissues. Primarily using wire, cluster and lattice deformers, digital models were systematically altered within Maya to re-create the ordered steps of each craniofacial procedure. Surgical tools were imported into Maya for use in the animations using computer-aided manufacturing files obtained directly from the manufacturer. The perspective of the virtual camera was liberally altered in combination with the tissue transparency capability in Maya to illustrate critical anatomic relationships pertinent to the surgeries.
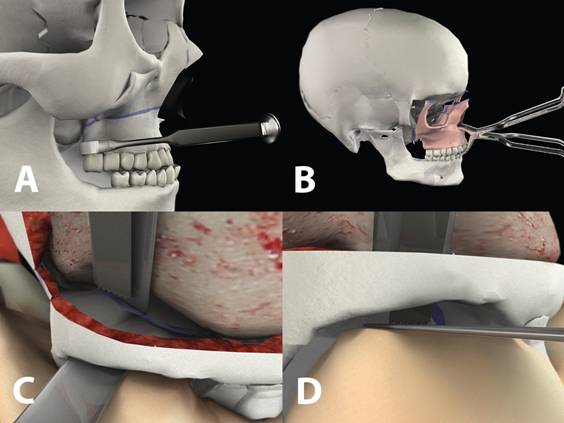
Results – Eight craniofacial procedures were animated in Maya: Genioplasty, Bilateral Sagittal Split Osteotomy, Intraoral Vertical Ramus Osteotomy, Lefort I, Mandibular Distraction, Transport Distraction, Fronto-Orbital Advancement with Cranial Vault Remodeling, Lefort III Advancement/Distraction, and Monobloc Advancement/Distraction. All surgical animations follow a systematic format in which the pathologic anatomy is reviewed, the pertinent surgical anatomy is displayed, and the procedure is performed. All major steps of the operative procedure are demonstrated, including exposure, execution of the osteotomy, displacement of the bone composite, and the predicted morphologic changes to the face. Throughout the surgical animation, the surgeon's operating room view is incorporated to reproduce the vantage of the surgeon. At various points during the animation, overlying tissue is rendered transparent to illustrate critical underlying anatomic relationships.
Conclusions – The first comprehensive virtual surgical atlas of craniofacial procedures is presented. These animations will serve as a constructive resource for trainees as well as practicing surgeons.