
Room 2 (Henry B. Gonzalez Convention Center)
Sunday, November 3, 2002
8:00 AM - 4:00 PM
Room 2 (Henry B. Gonzalez Convention Center)
Monday, November 4, 2002
8:00 AM - 4:00 PM
Room 2 (Henry B. Gonzalez Convention Center)
Tuesday, November 5, 2002
8:00 AM - 4:00 PM
Room 2 (Henry B. Gonzalez Convention Center)
Wednesday, November 6, 2002
8:00 AM - 4:00 PM
433
P2 - Aggressive Surgical Resection and Reconstruction for Locally Recurrent and Locally Advanced Breast Cancer
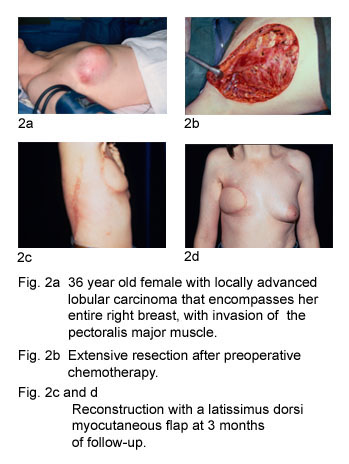
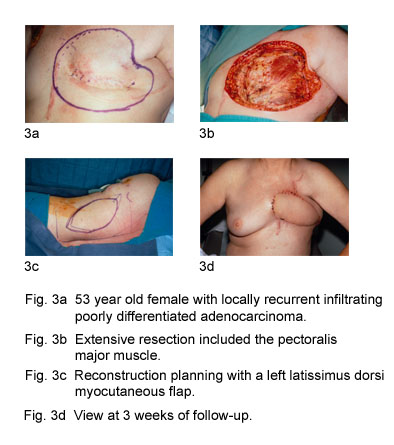
Surgical treatment of breast cancer has continue to become less extensive and invasive while still alowing for excellent control of local disease. However, a minority of women will still develop locally recurrent breast cancer or will present with locally advanced primary breast cancer. In some of these selected situations, aggressive surgical resection and reconstruction may be the only hope for attaining local control of the disease. In ten selected patients (7 with locally recurrent breast cancer and 3 with locally advanced primary breast cancer), we performed aggressive surgical resection followed by various methods of reconstruction: latissimus dorsi myocutaneous flap(7); latissimus dorsi myocutaneous flap plus tissue expander and implant(1); inframammary extended pectoralis major myocutaneous flap(1) and split thickness skin graft(1). No major postoperative complications occurred. Only minor wound healing problems were seen in 3 patients. Two of the 10 patients developed a local recurrence on their chest wall. Both went on to develop distant metastatic disease. A total of 5 patients developed distant metastasis within 2 to 16 months of their surgery. All 5 patients with distant metastatic disease died within 5 to 18 months of their procedure. Five of the 10 patients are still alive at follow-up periods ranging from 3 to 16 years. All 5 of these patients remain free of disease. Reconstructive options may be limited by previous radiotherapy or by tumor involvement of the pectoralis major muscles or internal mammary vessels. Nevertheless, reconstruction in these cases can be achieved by the use of the omentum, free flaps, or a combination of techniques. In conclusion, potential long standing palliation, or even cure, in selected cases of locally recurrent breast cancer or in selected cases of locally advanced disease can be attained with an approach of aggressive surgical resection and reconstruction. 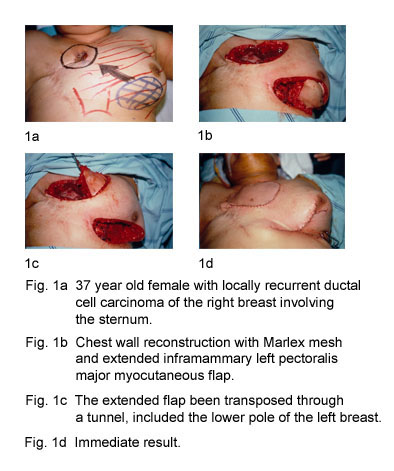
View Synopsis (.doc format, 176.0 kb)
See more of Posters
Back to 2002 Complete Scientific Program
Back to 2002 Meeting home