
Room 2 (Henry B. Gonzalez Convention Center)
Sunday, November 3, 2002
8:00 AM - 4:00 PM
Room 2 (Henry B. Gonzalez Convention Center)
Monday, November 4, 2002
8:00 AM - 4:00 PM
Room 2 (Henry B. Gonzalez Convention Center)
Tuesday, November 5, 2002
8:00 AM - 4:00 PM
Room 2 (Henry B. Gonzalez Convention Center)
Wednesday, November 6, 2002
8:00 AM - 4:00 PM
973
P5 - Anterolateral Thigh Flap: Anatomical Study of the Brazilian Population and Clinical Application
Abstract
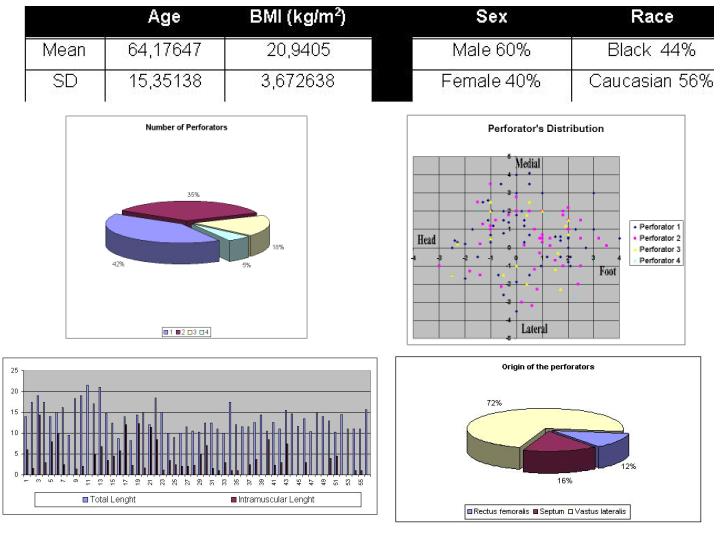
The anterolateral thigh flap was first described by Song, in 1984 (4), as a fasciocutaneous flap. Since the development of the perforator flaps by Kroll in 1988 (9) and Koshima in 1989 (2,8), many studies have been made, concluding that the majority of the anterolateral flaps did not have a septocutaneous pedicle. These flaps were nourished by muscle perforating vessels from lateral circumflex artery descent branch. (4,5,6,7). The aim of this paper was to study our population anatomy of anterolateral flaps and to report our experience in clinical practice. Fifty-eight anterolateral regions were dissected in twenty-nine fresh cadavers (table 1). The number of perforators found ranged from 1 to 4 in each dissected leg(Graphic 1). The majority of vessels were distributed around the middle point between the superior iliac spine and the patella’s lateral edge (graphic 2). Pedicles presented an average length of 13,48 cm and an average intramuscular path of 4,46 cm (graphic 3). The majority of the perforators coursed toward the vastus lateralis muscle (72%), while only 16% of the perforators had a septal course (graphic 4). The mean artery diameter was 2,55 mm and mean vein diameter was 3,47 mm. From December 2000 to January 2002, 29 flaps were used in the clinical series, with 1 ( one ) complete failure (3 %) due to kinking of the pedicle. No partial loss was observed. The largest flap dimension was 40 x15 cm and was based in 2 perforators. Flaps as wide as 10 cm could be used with primary closure of the donor area. Our anatomical study showed a similar anatomy of the brazilian population when compared with the asian population described in previous studies. Although there is a quite variable distribution of the perforators, we believe that the anterolateral thigh flap is reliable and has minor donor area deficit.
View Synopsis (.doc format, 616.0 kb)
See more of Posters
Back to 2002 Complete Scientific Program
Back to 2002 Meeting home