
Sunday, October 10, 2004
5713
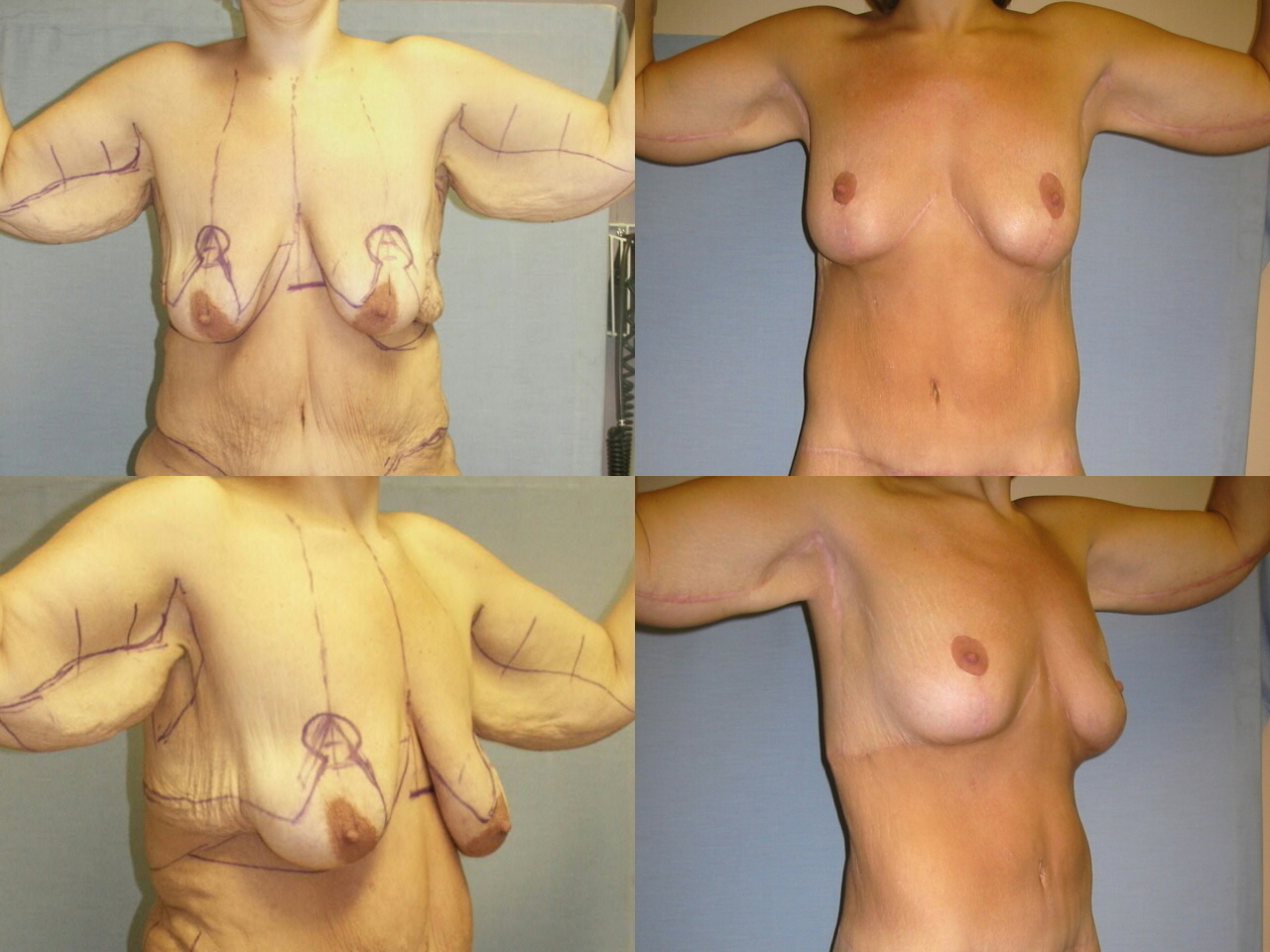
Breast Reshaping After Massive Weight Loss
Introduction: After massive weight loss, the breasts have poor shape, projection and skin elasticity. The nipples are distorted and ptotic. Mastopexy is recognized as difficult and may require excess nearby tissues. As the senior author’s approach evolved over the past 4 years, breast reshaping became integral to an upper body lift. This is a retrospective review of 24 patients Materials and methods: After the weight loss is stable, body contouring surgery has been performed on 74 patients. Six patients had mastopexy and /or augmentation only. Eighteen patients had breast reshaping as part of an Upper Body Lift. Follow up was from 2 to 46 months. This lift is a reverse abdominoplasty that ends along the inframammary fold incision of the Wise pattern mastopexy and continues laterally to along the back roll. When the breasts need enlargement, discard tissue from the epigastrium and lateral back roll is deepithelialized and used for augmentation. These flap extensions of the central breast pedicle spiral around the breast. (See Figure) When more tissue is needed, saline filled silicone implants have been used. The long inframammary incision forms the junction between the breast and reverse abdominoplasty. Secure inframammary fold construction along the sixth rib is pivotal to the Upper Body Lift and stability to the breast shape. Results: One smoking patient had limited skin necrosis and required debridement and skin grafting, which was later excised. Three patients had minor scar and contour correction. Two patients had secondary silicone implant augmentation. The remaining 18 patients were satisfied with their initial result. Conclusion: In the massive weight loss patient, breast reshaping is effectively and safely performed with an upper body lift. The upper body lift offers unique options to assist in reshaping the breast.
View Synopsis (.doc format, 61.0 kb)