Sunday, October 10, 2004
6084
Simplified Method of Ischial Pressore Sore Closure
The world's literature primarily emphasizes the importance of using flaps in closure of pressure sores. Residents are taught that flap surgery is the primary method to treat pressure sores if the patient is a surgical candidate. In addition, doctors of other specialties are impressed that a "flap" is needed when they cannot heal the pressure sore conservatively.
The authors in this presentation would like to change this mindset, that flaps are not always necessary in closing ischial pressure sores. We wish to erase this knee-jerk response in the surgical management of ischial pressure sores. The goal is management primarily should be focused on elimination of the ischial prominence, excision of scar tissue, and eradication of the focus of osteomyelitis. In majority of cases, adjacent soft-tissues, such as the proximal part of the hamstring muscles, can be advanced to close the wound without the need for formal flaps and major incisions.
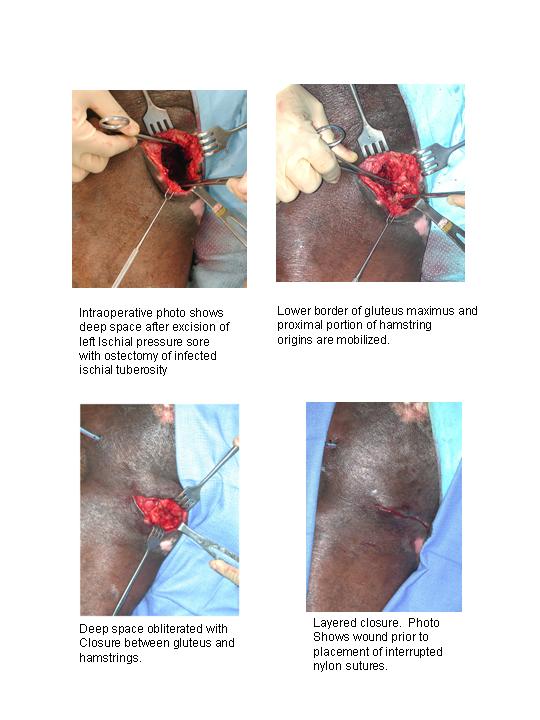
We report our series of 30 cases of ischial pressure sores using this protocol with successful closure in greater than 90% and a recurrence rate of less than 10% after an average of two years. The protocol requires an initial excision of the wound, including ischiectomy. After a period of dressing changes and bed rest, usually of one-week duration, further debridement is performed and the wound is closed by advancing the proximal part of the hamstrings. This is performed by minor extension of the initial incision, without major flap incisions (see figures).