
Sunday, October 28, 2007
12837
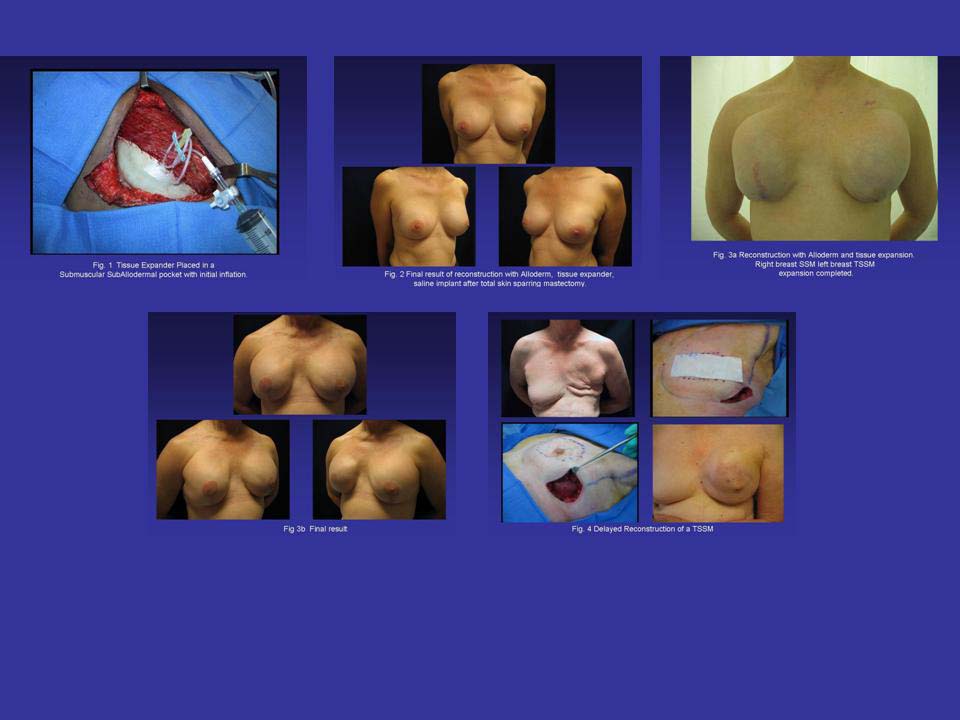
Three Year Experience with Alloderm in Breast Reconstruction
The addition of Alloderm to breast reconstruction has been of great versatility to solve a variety of tissue deficits. We describe our experience using Alloderm for 3 years (2004-2007) in 107 consecutive reconstructions with tissue expanders (TE) and saline implants.
Mastectomies were performed following carcinomas, sarcomas, or for prophylaxis. A sub-muscular, sub-Alloderm pocket accommodates a PMT-textured TE. Alloderm of medium thickness (12x4 cm) was positioned in the lateral border of the PM, infero-laterally as a sling, to reinforce portions of ablated muscle, or to increase nipple projection.
Results: 62 patients had 107 mastectomies, 60 (56%) following carcinoma, and 47 (43.9%) for prophylaxis. average age 49 (30-70). Total skin sparing: 90 cases (84.2%), skin sparing: 10 (9.3%), and modified radical 7 (6.5%). Op-time: 12min per Alloderm segment.
Complications: seromas (15.8%), hematomas (3.73%), cellulitis (3.7%), severe infection (5.6%) requiring TE removal, TE perforation (3.7%), TE lateral displacement (0.9%), local recurrence (0.9%), rippling (0.9%), and BII contracture (10%). Cosmetic score 8.5.
In conclusion, Alloderm has simplified breast reconstruction with TE, diminished the operative time and lowered the rate of complications. In addition, Alloderm provides a high rate of patient satisfaction and a significant increase in prophylactic mastectomies due to positive expectations.
View Synopsis (.doc format, 613.0 kb)