
Tuesday, October 30, 2007 - 8:10 AM
12868
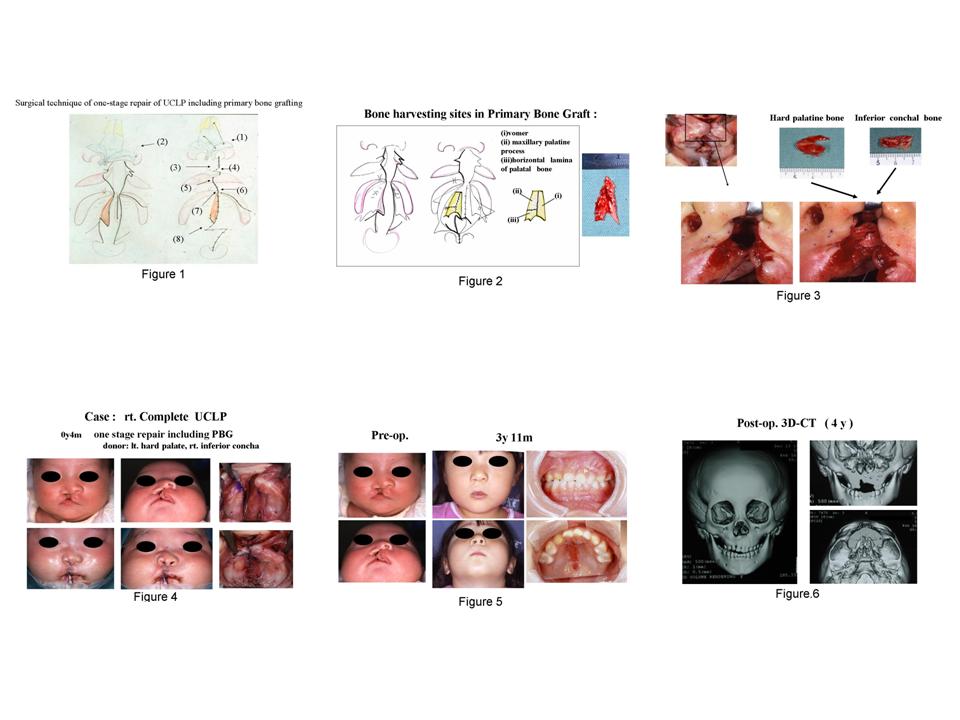
One Stage Repair of Cleft Lip and Palate including Primary Alveolar Bone Grafting
Purpose: Bone augmentation in alveolar cleft is very important in the treatment of cleft lip and palate. However, it remains challenging even in the unilateral cleft lip and palate. Some report that approximately 40% of UCLP patients required secondary bone grafting (SBG) even when they had succeeded in gingivoperiosteoplasty(GPP) after presurgical orthognathic treatment with Hotz plate, Latham appliance or Naso-Alveolar Molding(NAM) plate. As we have performed one-stage repair including primary alveolar bone grafting (PBG)for cleft lip and palate patients and gained good results, we present our technique and treatment outcome. Methods and Materials: Our cases are composed of totally 168 unilateral cleft lip and palate patients who underwent operation at the age between 3 to 9 months after presurgical orthognathic treatment from June 1998 to January 2006 in our hospital. Our one-stage repair technique includes (1)primary cleft rhinoplasty, (2)periosteoplasty of piriform aperture rim,(3)philtrumplasty (original method),(4)cheiloplasty by small triangle flap, (5)midline closure of vermillion, (6)gingivoperiosteoplasty(GPP) or gingivoperiosteoflap(GPF), (7)PBG from hard palate and/or inferior nasal concha ,and (8)palatoplasty by modified Furlow method using muco-periosteal flap of posterior nasal septum. (Fig.1) We have harvested hard palatal and/or inferior chonchal bone for PBG so that SBG will be unnecessary for almost all the cleft lip and palate patients. Our surgical technique of primary alveolar bone grafting from hard palate and/or inferior choncha is as follows. (a)Sagital mucosal incision is made on inferior choncha and chonchal bone is harvested under periosteum. (b)Hard palate is dissected under periosteum and palatal bone, maxillary bone and part of vomer are harvested. (Fig.2) (c)Harvested bone is not ground but curved to be grafted to alveolar cleft. (Fig. 3) Results: Shown in (Fig.4) is a female right complete unilateral cleft lip and palate patient,who underwent one-stage repair including primary alveolar bone grafting from left hard palate and right inferior concha at the age of 4 months in our hospital. (Fig.5) is a pre- and post-operative photos of her configuratuion and postoperative intraoral view. As postoperative CT images demonstrate,we have attained good bone formation. (Fig.6 ) Overall ,bone harvesting was possible in all the cases from hard palate and in some cases, we could not harvest the bone from inferior nasal concha because of poor view. So far, there have been no complications such as oro-nasal fistula or maxillary growth impairment and bone regeneration is observed in some cases, though incompletely. Discussion:In early 1900s,there were some papers reporting on surgical techniques of alveolar bone grafting with autologous bone such as the tibia,cranium,iliac crest,and ribs for the treatment of cleft lip and palate patients. In 1955,Nordin et al. and Schmid described PBG as a procedure for repair of alveolar defects in patients with cleft lip and palate using autologous rib at the time of cheiloplasty . In those days, PBG had been rather standard of care. However, in 1960s, there were opponents to PBG believing dissection of vomeromaxillary suture would bring about unfavorable results. Since Pruzansky reported that PBG resulted in midfacial growth impairment in 1964,PBG has become less and less popular .Today cleft lip and palate treatment trends favor the use of SBG instead. Recently,in spite of having been denied once historically,PBG has come to be reevaluated with the advancement of surgical technique and presurgical orthognathic treatment. In the background of our bringing back PBG,there are developments of palatoplasty of our modified Furlow method,which does not leave raw surface or maxillary growth impairment behind, GPP/GPF,and our own original sites for bone harvesting,that is ,hard palate and inferior nasal concha.Conclusion: Periosteum in infants has good potential of bone formation. We assume that harvested bone plays an important role as spacer in maintaining the shape of periosteum and that hard palate and inferior nasal concha are proper donor sites of PBG in one stage repair of cleft lip and palate.
View Synopsis (.doc format, 528.0 kb)
See more of Cranio/Maxillofacial/Head & Neck
Back to 2007am Complete Scientific Program